Redefining Risk: Enhancing Prognostic Assessment in Primary Prevention with Coronary Artery Calcium Score
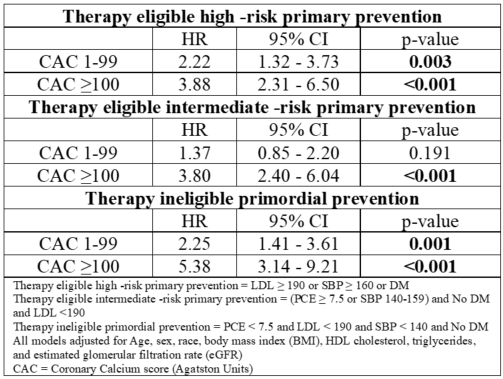
Abstract Body (Do not enter title and authors here): Introduction Current CV prevention strategies focus on treating individuals based on estimated risk or clinical thresholds, but risk heterogeneity exists even within treatment-eligible groups. Coronary artery calcium (CAC) scoring may enhance risk assessment, but its added value across the entire risk spectrum remains uncertain. Using data from a multiethnic population-based cohort, we examined the association of CAC burden with major adverse cardiovascular events (MACE). Methods Adults aged 45–64 years without baseline ASCVD from the Multi-Ethnic Study of Atherosclerosis (MESA) were included. Participants were categorized into three mutually exclusive risk groups based on baseline pooled cohort equation (PCE) scores, LDL, systolic blood pressure (SBP), and diabetes status: therapy eligible intermediate-risk primary prevention, therapy eligible high-risk primary prevention, and therapy ineligible primordial prevention. CAC was categorized as 0, 1-<100, and ≥100 Agatston units. Cox proportional hazards models were used to assess the association between CAC categories and incident MACE across risk groups, adjusting for age, sex, race, body mass index (BMI), HDL cholesterol, triglycerides, and estimated glomerular filtration rate (eGFR). MACE was defined as a composite of hard CVD events, coronary revascularization, and cardiovascular death. Results The cohort included 3,578 adults (mean age 54.6 years; 52.9% female; 27.6% African American), with a mean follow-up of 12.8 years. In fully adjusted models, higher CAC was independently associated with increased MACE risk across all risk groups. In the therapy eligible high-risk group, compared to CAC=0, the hazard ratio (HR) for CAC 1-99 was 2.22 (95% CI: 1.32-3.73; p=0.003) and 3.88 (95% CI: 2.31-6.50; p<0.001) for CAC ≥100. In the therapy eligible primary prevention group, HRs were 1.37 (95% CI: 0.85-2.19; p=0.191) for CAC 1-99 and 3.80 (95% CI: 2.40-6.04; p<0.0001) for CAC ≥100 (Table 1). In the therapy ineligible primordial prevention group, HRs were 2.25 (95% CI: 1.41-3.61; p=0.001) for CAC 1–99 and 5.38 (95% CI: 3.14-9.21; p<0.0001) for CAC ≥100. Conclusion Among treatment-eligible and ineligible adults, CAC provided independent and incremental prognostic information for MACE risk across the risk spectrum. These findings support the potential role of CAC testing to further individualize preventive strategies beyond traditional risk scores in both lower and higher risk populations.
Jindal, Sanmit
(
Houston Methodist
, Houston , Texas , United States )
Shahid, Izza
(
Houston Methodist
, Houston , Texas , United States )
Siddharth, Aditya
(
Houston Methodist Hospital
, Houston , Texas , United States )
Gullapelli, Rakesh
(
Houston Methodist
, HOUSTON , Texas , United States )
Javed, Zulqarnain
(
Houston Methodist
, Houston , Texas , United States )
Al Rifai, Mahmoud
(
Houston Methodist
, Houston , Texas , United States )
Al-kindi, Sadeer
(
Houston Methodist
, Houston , Texas , United States )
Nasir, Khurram
(
Houston Methodist
, Houston , Texas , United States )
Author Disclosures:
Sanmit Jindal:DO NOT have relevant financial relationships
| Izza Shahid:No Answer
| Aditya Siddharth:DO NOT have relevant financial relationships
| Rakesh Gullapelli:No Answer
| Zulqarnain Javed:DO NOT have relevant financial relationships
| Mahmoud Al Rifai:No Answer
| Sadeer Al-Kindi:No Answer
| Khurram Nasir:No Answer