Intersecting Inequities: Mapping Racial and Social Vulnerability Hotspots in U.S. Cardiogenic Shock Mortality
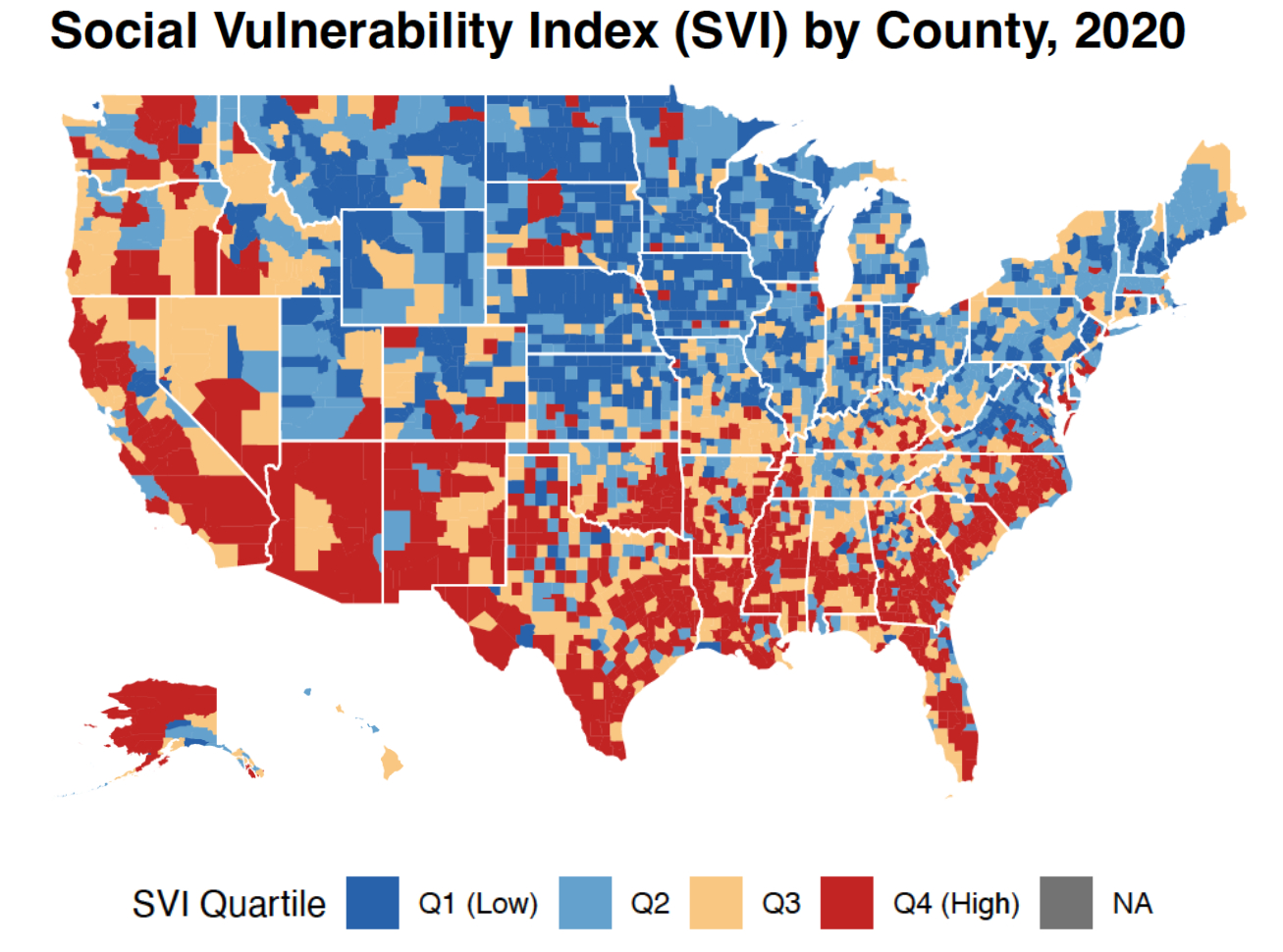
Abstract Body (Do not enter title and authors here): Background Cardiogenic shock [CS] remains highly lethal. Whether county-level structural vulnerabilities, as captured by the CDC Social Vulnerability Index [SVI], modify racial mortality gaps is unknown.
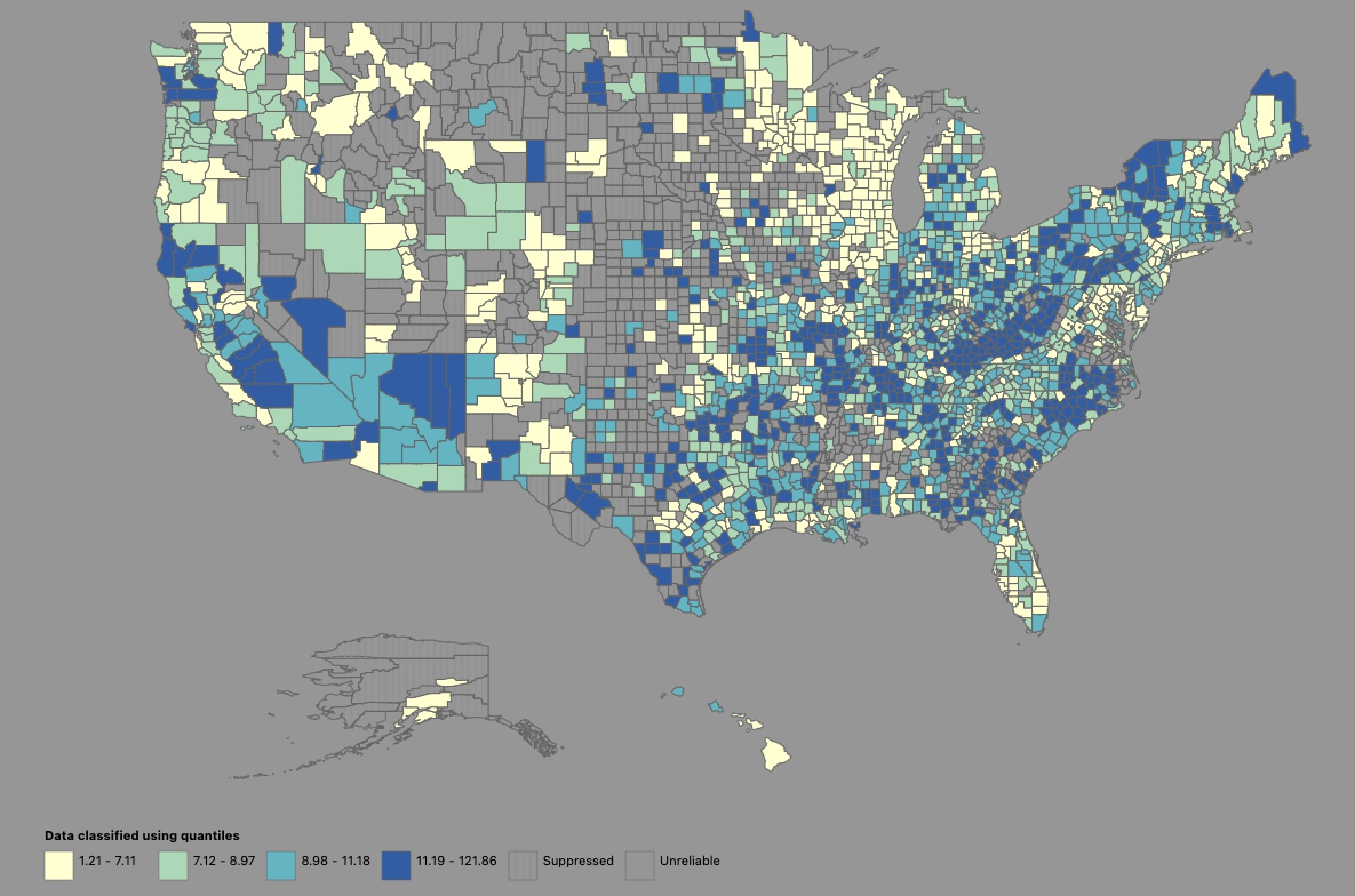
Objective To quantify area-specific CS mortality gradients across SVI quartiles and to map high-burden hotspots.
Methods We extracted mortality data about CS from CDC WONDER [2016–2020] and merged it with 2020 CDC SVI data. Age-adjusted mortality rates [AAMRs, per 100,000] were calculated for American Indian/Alaska Native [AIAN], Asian/Pacific Islander [API], Black, Hispanic, and White populations stratified by SVI quartile [Q1 being least, Q4 being most vulnerable]. One-way ANOVA tested AAMR differences across quartiles [alpha equal to 0.05]. Counties in Q4 whose race-specific AAMR exceeded the 95th percentile were designated hotspots.
Results We identified 22,051 CS deaths nationally. AAMRs increased stepwise from Q1 to Q4 for API [7.2 to 9], Black [12.1 to 14.3], Hispanic [7.5 to 11.2], and White [8.9 to 11.5] populations; gradients were significant for Hispanics [F= 4.54, P =0.004] and Whites [F=13.2, P < 0.001] but not for Blacks or APIs. AIAN individuals experience uniformly high AAMRs with no SVI gradient [F= 0.04, P= 0.97]. Hotspots clustered in rural high-SVI counties of the South and Southwest: Russell County, AL [AAMR 149.1 for Blacks; 121.9 for Whites], Carter County, OK [69.1 for AIAN], and Navajo/Apache Counties, AZ [59.44 Hispanics].
Conclusions County-level social vulnerability intensifies CS mortality for most racial groups, with steep gradients among Hispanic and White populations, while AIAN communities face persistently high risk irrespective of SVI. Race-SVI hotspot mapping pinpoints rural Southern and Southwestern counties where equitable access to timely revascularization, advanced heart failure therapies, and community-based prevention should be prioritized.
Luthra, Gaurav
(
Central Michigan University
, Saginaw , Michigan , United States )
Mohammed, Adil
(
Central Michigan University
, Saginaw , Michigan , United States )
Christian, Cleris
(
Central Michigan University
, Saginaw , Michigan , United States )
Singh, Sachin
(
Central Michigan University
, Saginaw , Michigan , United States )
Khan, Afrasayab
(
Central Michigan University
, Saginaw , Michigan , United States )
Ishfaq, Lyluma
(
Central Michigan University
, Saginaw , Michigan , United States )
El-hajj, Jad
(
Central Michigan University
, Saginaw , Michigan , United States )
Yasmeen, Umera
(
Mamata Medical College
, Khammam , India )
Beeharry, Sarah
(
Central Michigan University
, Saginaw , Michigan , United States )
Gariaqoza, Yousif
(
Central Michigan University
, Saginaw , Michigan , United States )
Do, Pauline
(
Central Michigan University
, Saginaw , Michigan , United States )
Mohammed, Zaki Ur Rahman
(
Sanford Health
, Moorhead , Minnesota , United States )
Kambali, Shrinivas
(
MyMichigan Health
, Saginaw , Michigan , United States )
Author Disclosures:
Gaurav Luthra:DO NOT have relevant financial relationships
| Yousif Gariaqoza:DO NOT have relevant financial relationships
| Pauline Do:DO NOT have relevant financial relationships
| Zaki Ur Rahman Mohammed:No Answer
| Shrinivas Kambali:No Answer
| Adil Mohammed:DO NOT have relevant financial relationships
| Cleris Christian:DO NOT have relevant financial relationships
| Sachin Singh:DO NOT have relevant financial relationships
| Afrasayab Khan:DO NOT have relevant financial relationships
| lyluma ishfaq:DO NOT have relevant financial relationships
| Jad El-Hajj:DO NOT have relevant financial relationships
| Umera Yasmeen:DO NOT have relevant financial relationships
| Sarah Beeharry:No Answer