Association between Pressure-Adjusted Heart Rate and Mortality in Cardiogenic Shock
Abstract Body (Do not enter title and authors here): Introduction: Among patients with cardiogenic shock (CS), high right atrial pressure (RAP) and low mean arterial pressure (MAP) are associated with in-hospital mortality. Pressure-adjusted heart rate (PAHR), defined as heart rate * RAP-to-MAP ratio (HR * [RAP/MAP]), integrates these parameters and has been used to identify cardiovascular dysfunction in critical illness. Higher PAHR values associate with higher surgical ICU mortality, but the prognostic significance of PAHR has not been assessed in cardiac intensive care unit (CICU) patients with CS.
Hypothesis: We hypothesized that higher PAHR values are associated with higher risk of in-hospital mortality in patients with CS.
Methods: The Critical Care Cardiology Trials Network (CCCTN) is a multinational registry of CICUs coordinated by the TIMI Study Group. Among CS admissions (2018-2023) undergoing invasive hemodynamic assessment within 24h of CICU admission, we calculated PAHR (in bpm) and assessed its relationship with in-hospital mortality. Patients on temporary mechanical circulatory support were excluded. Odds ratios were adjusted for age, sex, vasoactive-inotropic score (VIS), SCAI stage, and preceding cardiac arrest. Subgroup analyses stratifying by CS subtype were performed.
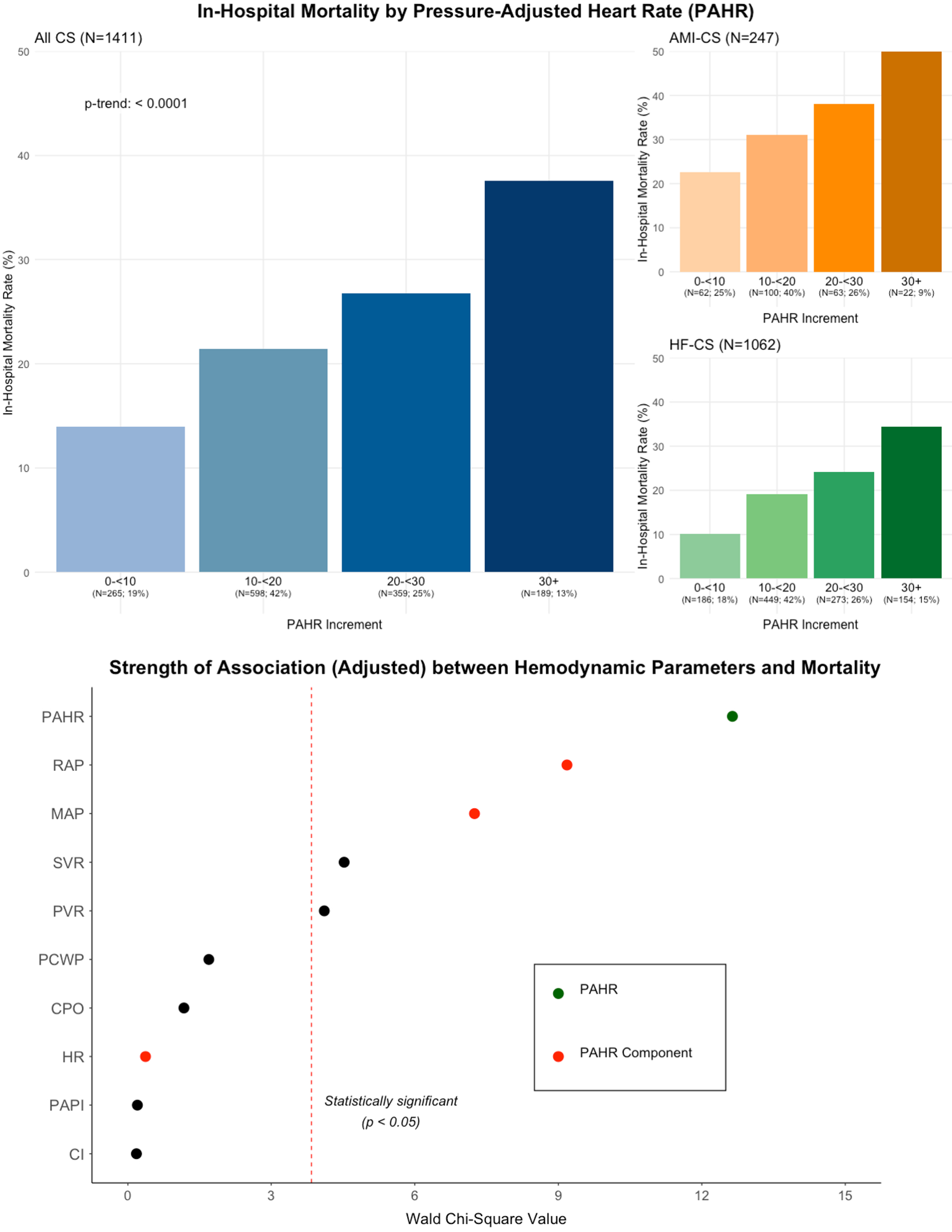
Results: Among the 1411 CS admissions in the analysis cohort (mean age 61 years, 31% women), 18% had AMI-CS, 75% had HF-CS, and 7% had secondary CS. At the time of assessment (median 1.4h after CICU admission), 75% were on vasoactive support (median VIS 3.8). Median HR was 92 (Q1-Q3 77-109) bpm, RAP 15 (Q1-Q3 10-19) mmHg, MAP 75 (Q1-Q3 67-87) mmHg, and PAHR 17 (Q1-Q3 11-24) bpm. A stepwise gradient of higher in-hospital mortality with increasing PAHR values (p-trend <0.001; Fig) was observed. In adjusted models, a higher PAHR was associated with higher in-hospital mortality (aOR per 10-bpm, 1.35 [95% CI, 1.15-1.58]), and had stronger prognostic associations with mortality than its individual hemodynamic components (Fig).
Conclusion: Higher PAHR is strongly associated with in-hospital mortality in CS patients. PAHR, a simple parameter which is readily calculable without needing a pulmonary artery catheter, may aid in identifying CS patients at higher risk of death.
Ginder, Curtis
(
Brigham and Women's Hospital
, Boston , Massachusetts , United States )
Jentzer, Jacob
(
Mayo Clinic
, Rochester , Minnesota , United States )
Guo, Jianping
(
Brigham and Women's Hospital
, Boston , Massachusetts , United States )
Van Diepen, Sean
(
UNIVERSITY OF ALBERTA
, Edmonton , Alberta , Canada )
Katz, Jason
(
NYU Langone
, New York , New York , United States )
Morrow, David
(
Brigham and Womens Hospital
, Boston , Massachusetts , United States )
Berg, David
(
Brigham and Womens Hospital
, Boston , Massachusetts , United States )
Author Disclosures:
Curtis Ginder:DO NOT have relevant financial relationships
| Jacob Jentzer:DO NOT have relevant financial relationships
| Jianping Guo:DO have relevant financial relationships
;
Other (please indicate in the box next to the company name):I am a member of the TIMI Study Group which has received institutional research grant support through Brigham and Women’s Hospital from: : Abbott, Abiomed, Inc., Amgen, Anthos Therapeutics, ARCA Biopharma, Inc., AstraZeneca, Boehringer Ingelheim, Daiichi-Sankyo, Ionis Pharmaceuticals, Inc., Janssen Research and Development, LLC, MedImmune, Merck, Novartis, Pfizer, Regeneron Pharmaceuticals, Inc., Roche, Saghmos Therapeutics, Inc., Softcell Medical Limited, The Medicines Company, Verve Therapeutics, Inc., Zora Biosciences:Active (exists now)
| Sean Van Diepen:DO NOT have relevant financial relationships
| Jason Katz:DO have relevant financial relationships
;
Researcher:Abbott Corporation:Active (exists now)
; Other (please indicate in the box next to the company name):Abiomed, DSMB Member:Active (exists now)
; Speaker:Zoll Corporation:Past (completed)
| David Morrow:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Cleerly:Active (exists now)
; Research Funding (PI or named investigator):Softcell:Active (exists now)
; Consultant:Roche:Active (exists now)
; Research Funding (PI or named investigator):Roche:Active (exists now)
; Consultant:Merck:Active (exists now)
; Consultant:Regeneron:Active (exists now)
; Research Funding (PI or named investigator):Regeneron:Active (exists now)
; Research Funding (PI or named investigator):Pfizer:Active (exists now)
; Research Funding (PI or named investigator):Novartis:Active (exists now)
; Research Funding (PI or named investigator):Daiichi Sankyo:Active (exists now)
; Research Funding (PI or named investigator):AstraZeneca:Active (exists now)
; Research Funding (PI or named investigator):Anthos Therapeutics:Active (exists now)
; Research Funding (PI or named investigator):Abiomed:Active (exists now)
; Consultant:Abbott:Active (exists now)
; Research Funding (PI or named investigator):Abbott:Active (exists now)
| David Berg:DO NOT have relevant financial relationships