Association Between Creatinine-to-Cystatin C Ratio, Subclinical Myocardial Injury, and Mortality: National Health and Nutrition Examination Survey
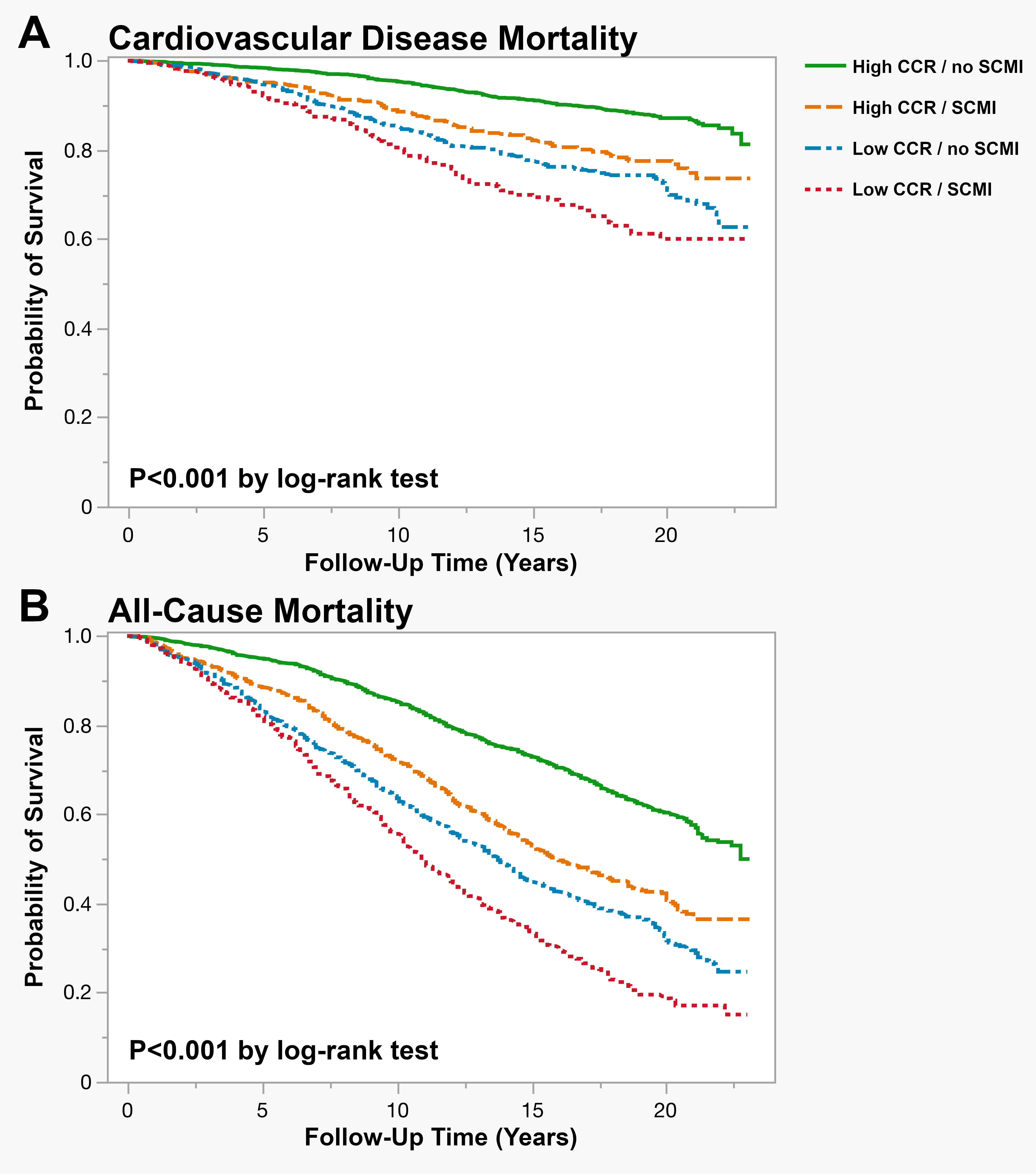
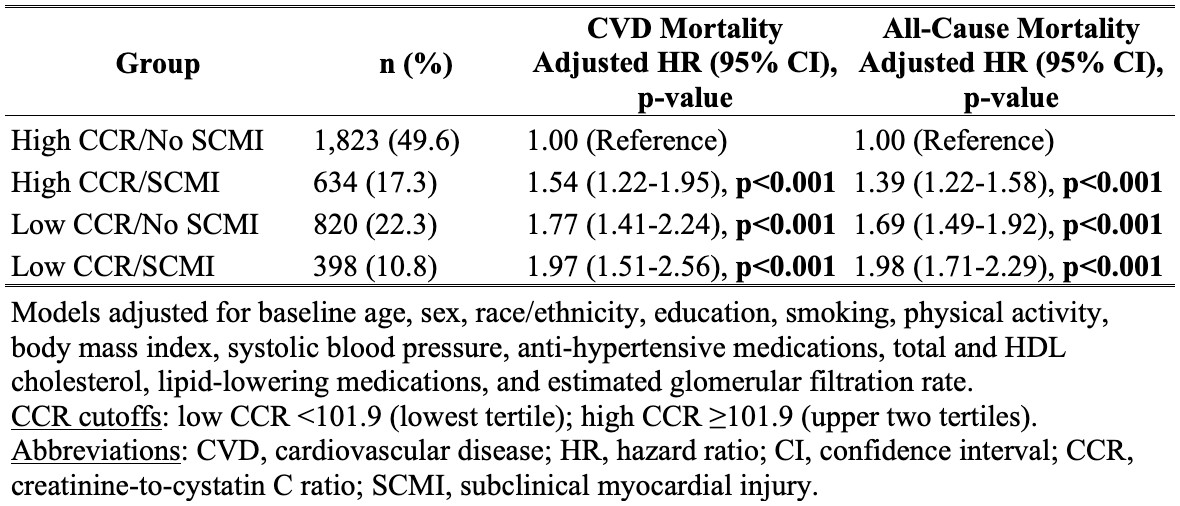
Abstract Body (Do not enter title and authors here): Background: The creatinine-to-cystatin C ratio (CCR) is an emerging biomarker of skeletal muscle health that predicts cardiovascular outcomes. Subclinical myocardial injury (SCMI) affects over 20% of adults and increases mortality risk. The relationship between CCR, SCMI, and mortality remains unexplored. Hypothesis: We hypothesized that: 1) Lower CCR would be associated with increased SCMI prevalence; 2) Both low CCR and SCMI would independently predict all-cause and cardiovascular disease (CVD) mortality; and 3) Participants with concurrent low CCR and SCMI would demonstrate the highest mortality risk. Methods: We analyzed NHANES III (1988-1994) participants aged ≥40 years who underwent electrocardiogram (ECG) recording, excluding those with CVD history, ECG evidence of myocardial infarction, estimated glomerular filtration rate (eGFR) <30 mL/min/1.73m2, or missing data. CCR was calculated as serum creatinine (mg/dL)/cystatin C (mg/L) x 100. SCMI was defined as a cardiac infarction injury score ≥10 on 12-lead ECG. Mortality was ascertained from the National Death Index. Multivariable logistic regression assessed the baseline cross-sectional association between CCR (z-score standardized) and the presence of SCMI. Cox Proportional Hazard models were used to examine the association of combined CCR and SCMI categories with mortality (low CCR: lowest tertile <101.9; high CCR: upper two tertiles ≥101.9). Models were adjusted for age, sex, race/ethnicity, education, smoking, physical activity, body mass index, systolic blood pressure, anti-hypertensive medications, total and HDL cholesterol, lipid-lowering medications, and eGFR. Results: Among 3,675 participants (mean age 64.8±12.4 years, 52.7% female), 1,032 (28.1%) had SCMI. Each 1-SD decrease in CCR was associated with 13% increased odds of SCMI (adjusted OR 1.13, 95% CI 1.02-1.25). During a median follow-up of 17.5 (9.9-19.6) years, 596 CVD deaths and 1,973 all-cause deaths occurred. Combined CCR-SCMI categories showed graded associations with mortality (Figure), with low CCR/SCMI showing the highest risk for both CVD mortality (adjusted HR 1.97, 95% CI 1.51-2.56) and all-cause mortality (adjusted HR 1.98, 95% CI 1.71-2.29) compared to high CCR/no SCMI (Table). Conclusions: Low CCR is associated with increased SCMI prevalence. They both independently predict mortality, with the combination showing the greatest risk.
Mirzai, Saeid
(
Wake Forest University SOM
, Winston Salem , North Carolina , United States )
Patel, Vraj
(
Wake Forest University SOM
, Winston Salem , North Carolina , United States )
Sandesara, Uttsav
(
Wake Forest University SOM
, Winston Salem , North Carolina , United States )
Chevli, Parag
(
Wake Forest University SOM
, Winston Salem , North Carolina , United States )
Mostafa, Mohamed
(
Wake Forest University SOM
, Winston Salem , North Carolina , United States )
Kazibwe, Richard
(
Wake Forest University SOM
, Winston Salem , North Carolina , United States )
Soliman, Elsayed
(
Wake Forest University SOM
, Winston Salem , North Carolina , United States )
Author Disclosures:
Saeid Mirzai:DO NOT have relevant financial relationships
| Vraj Patel:No Answer
| Uttsav Sandesara:DO NOT have relevant financial relationships
| Parag Chevli:DO NOT have relevant financial relationships
| Mohamed Mostafa:No Answer
| Richard Kazibwe:DO NOT have relevant financial relationships
| Elsayed Soliman:DO NOT have relevant financial relationships