Safety and Hemostatic Efficacy of Prothrombin Complex Concentrate Versus Fresh Frozen Plasma in Patients undergoing Cardiac Surgery: A Systematic Review and Meta-Analysis.
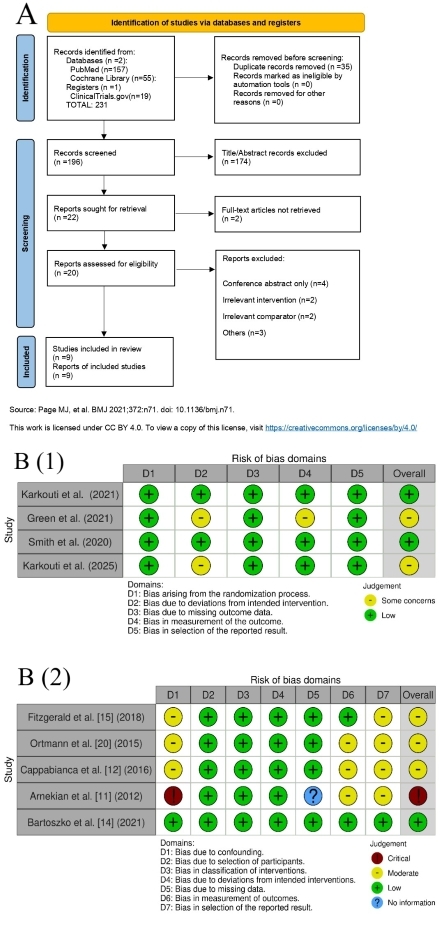
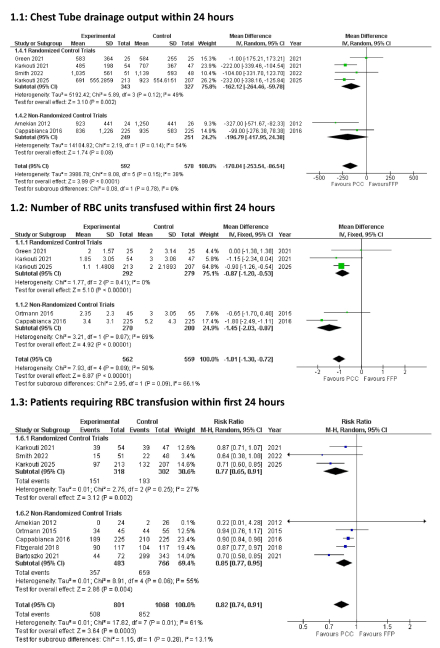
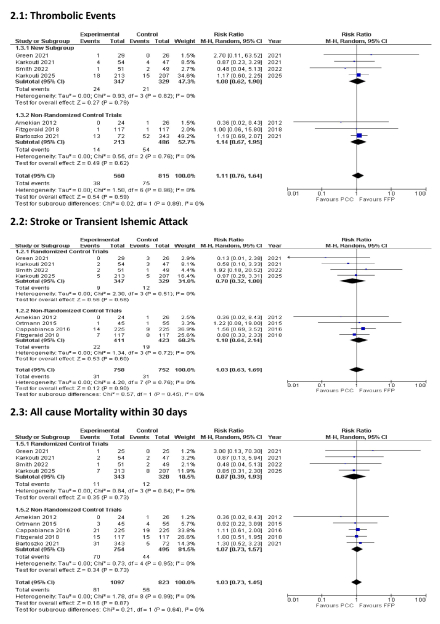
Abstract Body (Do not enter title and authors here): INTRODUCTION : In patients undergoing cardiac surgery, up to 15% experience major intraoperative and postoperative bleeding. Earlier research indicates excessive bleeding associated with cardiac surgery as an independent risk factor for increased morbidity and mortality. Prothrombin complex concentrate (PCC) and fresh frozen plasma (FFP) are frequently used to control the bleeding during cardiac surgery. METHODS : A comprehensive literature search was conducted using PubMed, Cochrane Library, and ClinicalTrials.gov to identify relevant randomized controlled trials and observational studies which directly compared PCC and FFP in patients undergoing cardiac surgery experiencing bleeding. The search terms included different keywords for “Prothrombin Concentrate Complex”, “Fresh Frozen Plasma” and “Cardiac Surgery”. After screening and eligibility assessment, 9 articles (4 RCTs and 5 observational studies) were included from an initial pool of 231 records. Meta-analysis was performed using RevMan 5.4 software. Quality assessment was performed using the Cochrane Risk of Bias tool for RCTs and Robbins-1 tool for observational studies. RESULTS: Final analysis included 1920 patients to investigate the relative effect of PCC vs FFP on 6 different efficacy and safety parameters in cardiac surgery patients.The pooled analysis demonstrated the efficacy of PCC in significantly reducing the chest tube drainage output within the first 24 hours postoperatively as compared to the FFP group (mean difference [MD] , -170.04 ml; 95% CI, -253.54 to -86.54 ml; p < 0.0001). When compared to the FFP group, the PCC group also had a significantly lower number of RBC units transfused ( MD, -1.01 units; 95% CI, -1.30 to -0.72 units; p < 0.0001) as well as number of patients needing RBC transfusion in the first 24 hours (RR, 0.82; 95% CI, 0.74 to 0.91;p=0.0003). Safety analysis showed no significant difference between the PCC and FFP groups for the parameters of Stroke or TIA (RR, 1.03; 95% CI,0.63 to 1.69; p=0.90), thromboembolic events (RR, 1.11; 95% CI,0.76 to 1.64; p=0.59) and all-cause mortality within 30 days (RR,1.03; 95 % CI, 0.73 to 1.45; p=0.87). DISCUSSION : In patients undergoing cardiac surgery with coagulopathy or bleeding, PCC was associated with improved hemostatic efficacy and reduced transfusion requirements compared to FFP. Importantly, these benefits were achieved without an increased risk of thromboembolic events, stroke, or mortality.
Akhter, Haji Abdul Rehman
(
CMH Multan Institute of Medical Sciences
, Mutan , Punjab , Pakistan )
Khan, Sheraz
(
Khyber Medical College Peshawar
, Peshawar , Pakistan )
Italiya, Kevin
(
GMERS medical college, Valsad
, Surat , India )
Senk Juh, Amadej
(
University of Ljubljana
, Ljubljana , Slovenia )
Khalid, Maliha
(
Jinnah Sindh Medical University
, Karachi , Pakistan )
Garg, Hanish
(
SUNY Upstate Medical University
, Syracuse , New York , United States )
Author Disclosures:
Haji Abdul Rehman Akhter:DO NOT have relevant financial relationships
| Sheraz Khan:DO NOT have relevant financial relationships
| Kevin Italiya:DO NOT have relevant financial relationships
| Shaurya Kamboj:DO NOT have relevant financial relationships
| Amadej Senk Juh:DO NOT have relevant financial relationships
| Maliha Khalid:DO NOT have relevant financial relationships
| Hanish Garg:DO NOT have relevant financial relationships