Patients with Acute Ischemic Stroke in the United States Exhibit more Dependency 90 Days after Stroke than those in a Matched Norwegian Cohort
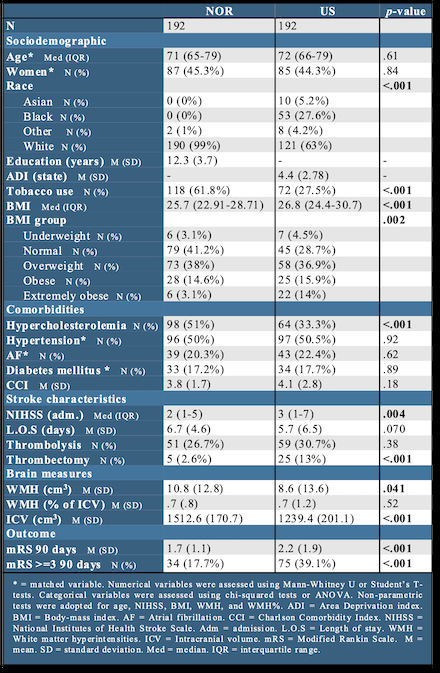
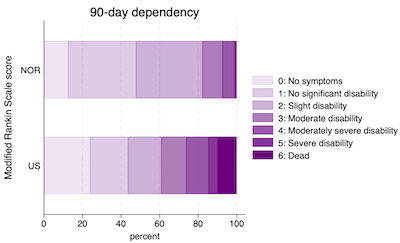
Abstract Body: Introduction: Acute ischemic stroke (AIS) imposes a disparate burden across global populations. Understanding drivers of such heterogeneity is particularly important in the context of international stroke clinical trials design. We sought to identify the differential clinical and neuroimaging characteristics, and outcomes in matched AIS cohorts from Norway (NOR) and the United States (US). Methods: AIS data was retrieved from the ‘Norwegian Cognitive Impairment After Stroke study (Nor-COAST; NOR) and the Registry for Neurological Endpoints among patients with Ischemic and Hemorrhagic Stroke(REINAH; US). White matter hyperintensities (WMH) and intracranial volumes (ICV) were extracted from MRI images by training a deep learning model, and the softwares FreeSurfer and FSL. Cohorts were matched on age, sex, diabetes, atrial fibrillation, and hypertension. We applied inferential statistics, as well as fit a logistic regression model to evaluate dependency (mRS >=3) in the cohorts, adjusting for age, sex, race, NIHSS, smoking, hypercholesterolemia, thrombolysis, thrombectomy, and ICV-normalized WMH. Results: A total of 384 matched AIS patients (192 in each cohort) were included. Demographic, clinical, and imaging characteristics along with outcomes are reported in fig. 1. The cohorts were not statistically different across the matched characteristics. Likewise, WMH burden was similar across cohorts. The NOR cohort had a significantly higher proportion of previous/current smokers and a higher prevalence of hypercholesterolemia. The US cohort had greater ethno-racial heterogenity, higher BMI, and higher NIHSS on admission. A greater proportion of the US cohort underwent IV thrombolysis (30.7% vs. 26.7%), however this difference was not statistically significant. Conversely, a significantly higher proportion of the US cohort received thrombectomies (13% vs 2.6%). The US cohort had higher levels of 90-day dependency (mRS≥3; fig. 2) as compared to NOR (39.1% vs. 17.7%). This difference translated into a significantly higher likelihood of 90-day dependency among the US patients (vs. NOR) in the fully adjusted model (OR = 2.28, 95% CI 1.23, 4.24). Conclusion: Cohorts from the US and Norway demonstrated significant differences in demographic, clinical, treatment profiles, and 90-day dependency after stroke. The differences may be driven by an interplay of demographic, genetic, healthcare system, socio-behavioral, and societal factors within the global stroke population.
Aamodt, Eva
(
Oslo University Hospital
, Oslo , Norway )
Rovang, Martin
(
Oslo University Hospital
, Oslo , Norway )
Beyer, Mona Kristiansen
(
Oslo University Hospital
, Oslo , Norway )
Macintosh, Bradley
(
Oslo University Hospital
, Oslo , Norway )
Potter, Thomas
(
Houston Methodist
, Houston , Texas , United States )
Vahidy, Farhaan
(
TIRR Memorial Hermann
, Houston , Texas , United States )
Author Disclosures:
Eva Aamodt:DO NOT have relevant financial relationships
| Martin Rovang:No Answer
| Mona Kristiansen Beyer:DO NOT have relevant financial relationships
| Bradley MacIntosh:DO NOT have relevant financial relationships
| Thomas Potter:DO NOT have relevant financial relationships
| Farhaan Vahidy:DO NOT have relevant financial relationships