Quantifying the Rising Burden of Heart Failure Due to Cocaine Use in High-Income Countries: A 34-Year Global Perspective
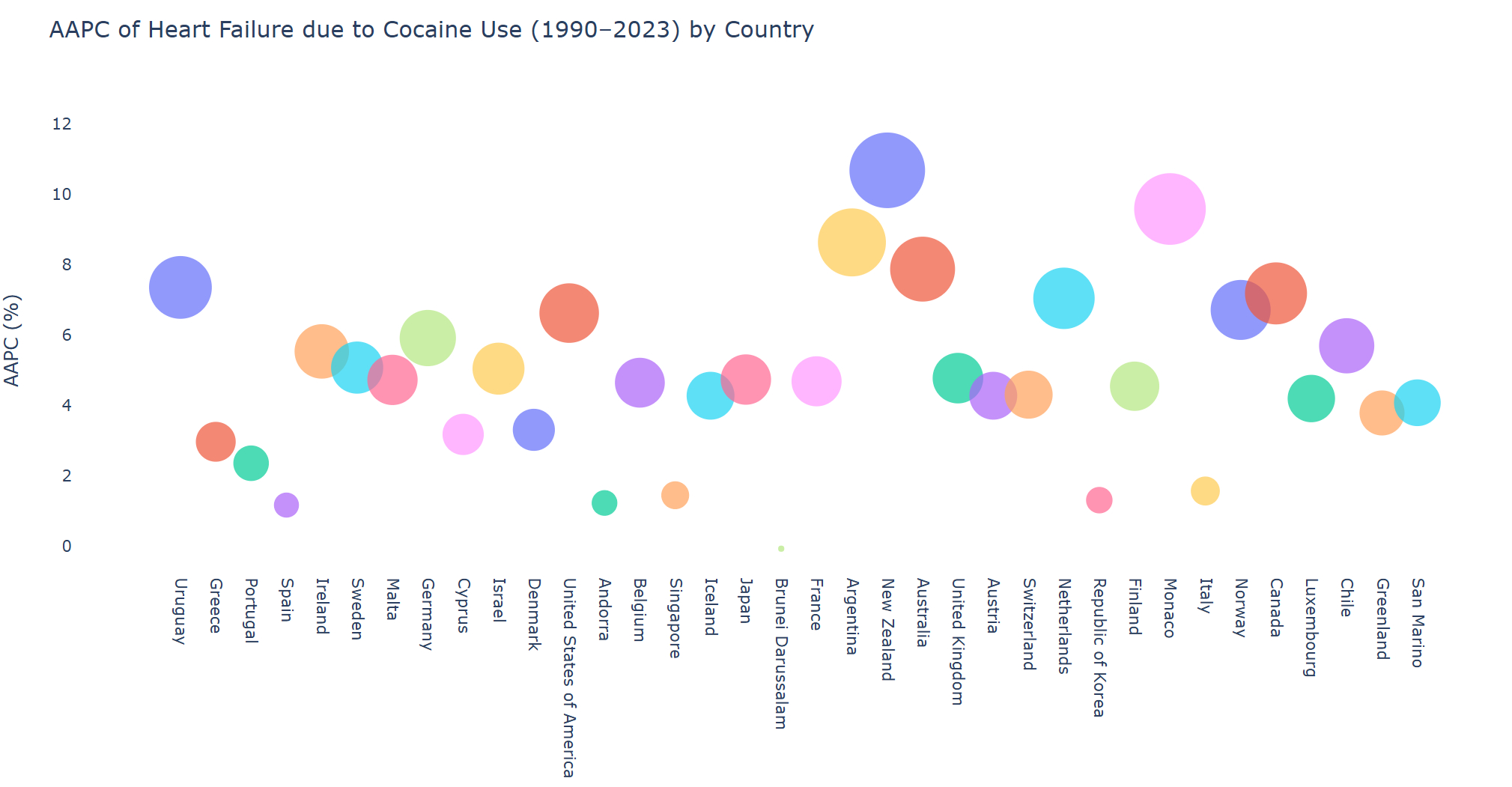
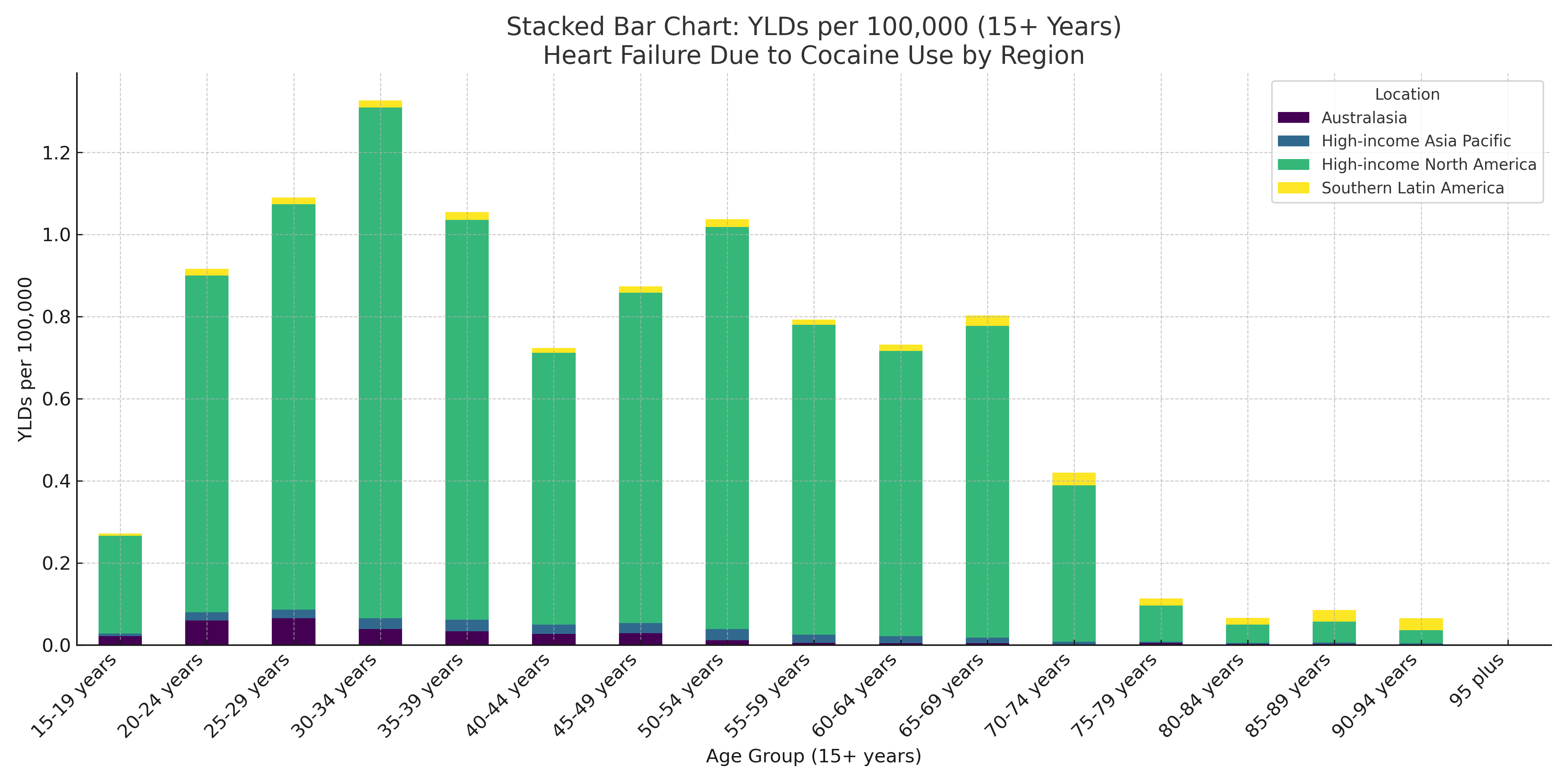
Abstract Body: Background: Cocaine use disorder (CUD) represents a significant, yet often underappreciated, public health challenge in high-income countries (HIC), contributing to substantial cardiovascular morbidity and mortality. Cocaine-associated cardiotoxicity can manifest as Cocaine-Induced Cardiomyopathy (CIC), ultimately leading to Heart Failure (HF). Method: We analyzed prevalence and years lived with disability (YLD) for HF due to CUD, using standardized GBD 2023 tool stratified by age, sex, year and location across HIC from 1990 to 2023. Cocaine exposure was estimated using DisMod-MR 2.1, a Bayesian meta-regression model. The burden attributable to cocaine was derived using the Comparative Risk Assessment framework, integrating exposure prevalence, relative risks, and theoretical minimum risk levels to calculate population-attributable fractions. Results: Between 1990 and 2023, the absolute number of prevalent cases of HF due to CUD increased from 3,028 to 8,608, while YLDs rose from 279.9 to 793.2 in HIC. The age-standardized prevalence rate increased significantly, with an AAPC of 7.07%, and the age-standardized YLD rate grew at 7.08%. Region-wise, the highest AAPC in prevalence was observed in Australasia (8.05%), followed by High-income North America (HINA) (6.71%), Southern Latin America (6.68%), Western Europe (4.39%), and High-income Asia Pacific (3.36%). The peak burden of HF YLDs due to cocaine use was observed in the 30-34 year age group, reaching approximately 0.51 YLDs per 100,000 population while prevalence rate 5.53 per 100,000 in 2021. HINA was the dominant regional contributor, accounting for over 85% of the total YLDs in the young-to-middle-aged adult population in 2021. Sex-wise trends showed that males had a higher AAPC in YLDs (6.17%), while females showed slightly higher AAPC in prevalence (6.17%) vs. males (5.60%), indicating differing trajectories in disability progression and healthcare utilization. Conclusion: HF attributable to CUD has escalated significantly in HIC over the past three decades, with HINA consistently contributing the highest burden. Australasia showed the steepest rise in prevalence, while the peak disability occurred in adults aged 30–34 years. Males experienced greater YLD progression, whereas females showed a faster rise in prevalence.
Parisapogu, Anusha
(
University of Connecticut
, Hartford , India )
Varma, Revati
(
Cook County Health
, Chicago , Illinois , United States )
Sudan, Sourav
(
St Vincent Hospital,
, Worcester , Massachusetts , United States )
Vummaneni, Siri
(
Detroit Medical Center/Wayne State University.
, Detroit , Michigan , United States )
Sami, Shahzad Ahmed
(
DCH RMC/university of Alabama
, Tuscaloosa , Alabama , United States )
Gera, Asmita
(
Maimonides medical Center, Brooklyn,
, Brooklyn , New York , United States )
Yedida, Naga Teja
(
Rangaraya Medical College,
, Kakinada , Andhra Pradesh , India )
Gujjari, Sindhu
(
Northwestern Medicine Mchenry Hosp
, Mchenry , Illinois , United States )
Parul, Fnu
(
U of M Health- Sparrow Hospital
, Lansing , Michigan , United States )
Desai, Hardik Dineshbhai
(
Independent Public Health Researcher
, Ahmedabad , Gujarat , India )