Global Impact of Tobacco Control Policies on Cardiovascular Mortality: A Lag-Adjusted Fixed-Effects Analysis of 148 Countries (2007–2022)
Abstract Body: Background: Tobacco use remains a leading modifiable driver of cardiovascular disease (CVD) worldwide. The WHO MPOWER framework quantifies national tobacco-control strength, yet longitudinal causal associations with CVD mortality have not been comprehensively quantified across countries. Methods: A longitudinal panel of 148 countries (2007–2022) was assembled integrating: (1) Global Burden of Disease 2023 estimates of age-standardized CVD mortality attributable to tobacco (per 100 000); (2) WHO MPOWER composite scores (0–5 scale, equal-weighted across six policy components); and (3) World Bank GDP per capita (USD). We applied country- and year-fixed-effects linear regression to estimate the association between MPOWER intensity at t–3 and subsequent CVD mortality at year t, adjusting for log-transformed GDP. The three-year lag was selected a priori, consistent with cardiovascular disease latency periods. Robust (HC3) standard errors were clustered by country. Sensitivity analyses tested alternate lag structures (t–1 to t–5), exclusion of outliers (±3 SD or high Cook’s distance), and GDP-by-income-level interaction terms.
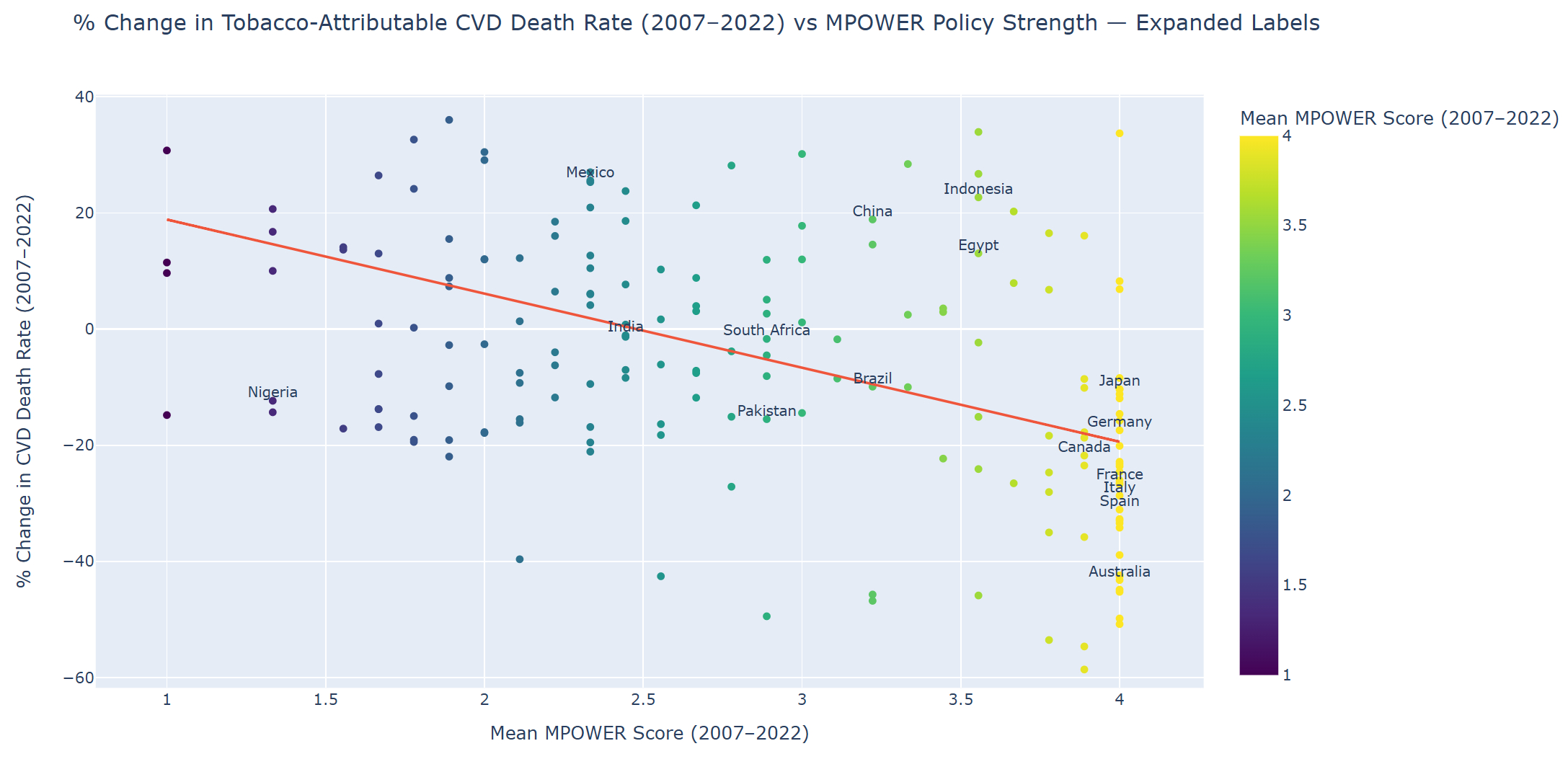
Results: From 2007–2022, global tobacco-attributable CVD mortality declined from 37.3 to 32.4 per 100 000 (–13.2%), as mean MPOWER strength increased from 2.7 to 2.9. Each one-point increase in lagged MPOWER score was associated with a 1.07 ± 0.20 per 100 000 reduction in CVD mortality (p < 0.001), independent of GDP (β = –2.10 ± 0.69; p = 0.002). Over the full MPOWER scale (0→5), this translates to ~5.4 fewer deaths per 100 000, representing a 16% decline at mean baseline mortality. A 1% increase in GDP corresponded to a 0.021 per 100 000 reduction in CVD mortality. Model fit was strong (within-country R2 = 0.71; total R2 = 0.97). Income-level interactions were non-significant, indicating consistent MPOWER effects across development contexts. High-policy countries (UK, Australia, Japan, Brazil) achieved steepest declines, while lower-policy countries (Nigeria, Ethiopia, Pakistan) showed limited progress. Conclusions: Stronger MPOWER implementation, sustained over multiple years, is independently associated with substantial reductions in tobacco-attributable CVD mortality worldwide, even after accounting for GDP, year effects, and lag structure. While residual confounding and ecological inference limit causal certainty, these findings provide robust, policy-relevant evidence supporting global intensification of comprehensive tobacco control.
Parisapogu, Anusha
(
University of Connecticut
, Hartford , India )
Desai, Hardik Dineshbhai
(
Independent Public Health Researcher
, Ahmedabad , Gujarat , India )
Gera, Asmita
(
Maimonides medical Center,
, Brooklyn , New York , United States )
Sami, Shahzad Ahmed
(
DCH RMC/university of Alabama
, Tuscaloosa , Alabama , United States )
Parul, Fnu
(
U of M Health- Sparrow Hospital
, Lansing , Michigan , United States )
Gunani, Manas
(
Allegheny Health Network
, Pittsburgh , Pennsylvania , United States )
Vummaneni, Siri
(
Detroit Medical Center/Wayne State University. 4201 St. Antoine St Detroit,
, Detroit , Michigan , United States )
Varma, Revati
(
Cook County Health
, Chicago , Illinois , United States )
Sudan, Sourav
(
St Vincent Hospital,
, Worcester , Massachusetts , United States )
Yedida, Naga Teja
(
Rangaraya Medical College,
, Kakinada , Andhra Pradesh , India )