Spatiotemporal Restructuring of United States Atherosclerosis Mortality and the Emerging Distribution of Cardiometabolic Risk
Abstract Body: Background: Geographic disparities in atherosclerotic cardiovascular disease (ASCVD) mortality are longstanding, yet the pandemic disrupted cardiometabolic care and population risk. Whether ASCVD mortality patterns reconfigured during this period and to what extent such changes reflect county-level cardiometabolic burden versus age structure remain unclear.
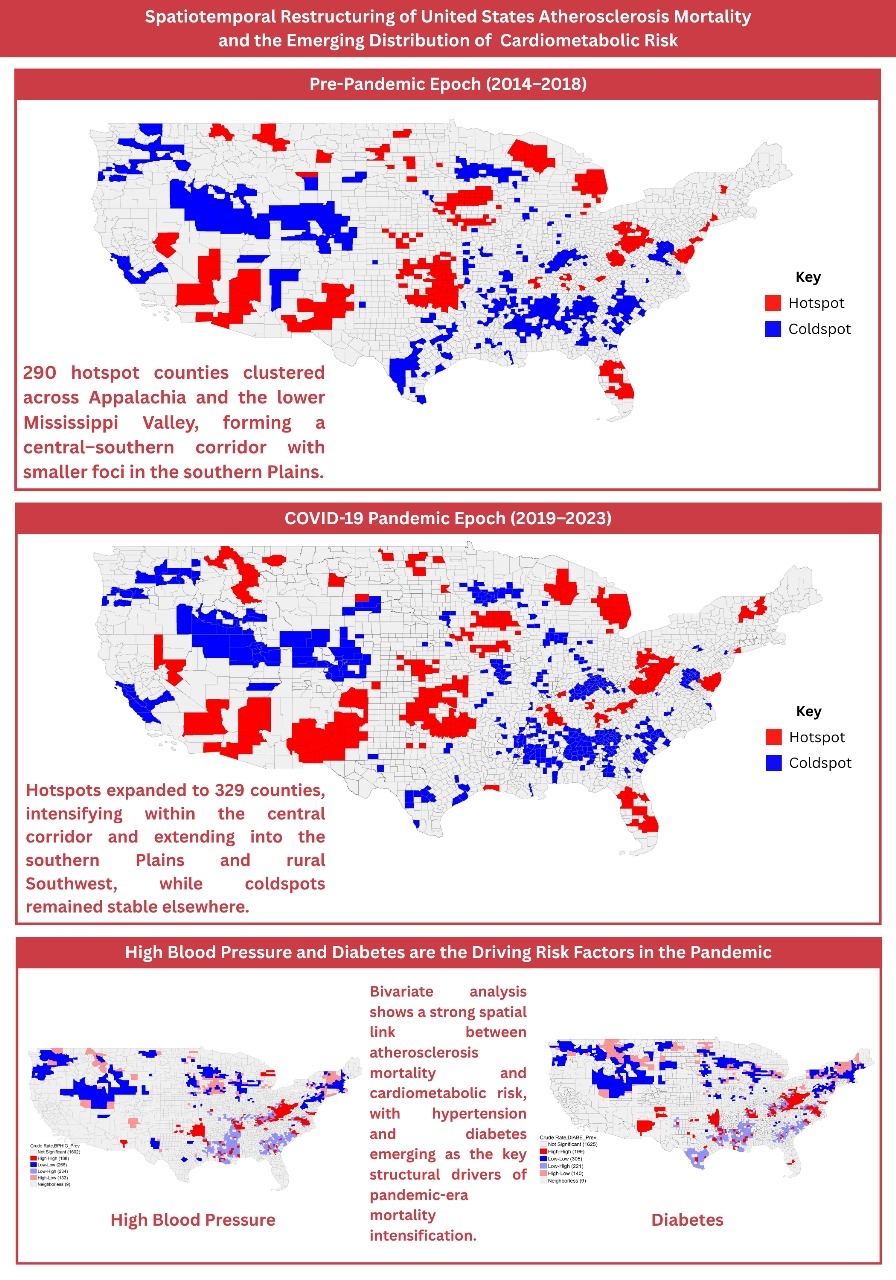
Methods: A retrospective, county-level geospatial analysis of ASCVD mortality (ICD-10: I25.0, I25.1, I70) using CDC WONDER data, comparing pre-pandemic (2014–2018) and pandemic-era (2019–2023) epochs was conducted using crude mortality rates (CMR). Three risk factors, hypertension, diabetes, and high cholesterol were examined using CDC PLACES data. Analysed using GeoDa, univariate Getis-Ord Gi* (p<0.05) identified clusters, with bivariate Local Moran’s I evaluating spatial overlap between high-CMR clusters, risk factor prevalence, and median age to assess confounding.
Results: Between 2014–2018 and 2019–2023, U.S. atherosclerosis mortality restructured toward larger, more contiguous high-risk clusters spanning the Lower Mississippi Delta, Black Belt, and central–southern Appalachia, extending into Oklahoma and north-central Texas. Hotspots increased from 290 to 329 with mean CMR rising from 128.63 to 135.50, while coldspots remained stable (434→432; 53.18→53.76), indicating intensification within established regions rather than a national rise. Low-risk zones persisted across the Upper Midwest, Northern Plains, Mountain West, and coastal New England and Pacific areas. Age confounding was limited: hotspot–coldspot median age shifted modestly (42.55 vs. 38.80 to 43.13 vs. 39.52), and major clusters extended beyond the oldest counties. Bivariate overlays showed the strongest, increasingly coherent spatial concordance between mortality hotspots and diabetes clusters, secondary alignment with hypertension, and fragmented overlap with high cholesterol, suggesting pandemic-era mortality intensification was driven chiefly by diabetes, supported by hypertension, beyond aging effects.
Conclusion: U.S. atherosclerosis mortality geography has polarized, with widening divides between high- and low-risk regions. This reflects consolidation of the traditional Southeastern belt and emergence of a new mortality frontier in the South-Central U.S. The westward expansion appears closely linked to diabetes prevalence, marking a pivotal shift in the drivers of national cardiometabolic disparities.
Farooq, Minaam
(
South Texas Health System
, McAllen , Texas , United States )
Uddin, Muhammad Salik
(
Dow Medical College
, Karachi , Pakistan )
Mansoor, Areesha
(
Dow university of health sciences
, Karachi , Pakistan )
Khan, Ammaar Ali
(
Dow University of Health Sciences
, Karachi , Pakistan )
Abdullah, Muhammad
(
HCA Florida Oak Hill Hospital
, Brooksville , Florida , United States )
Elahi, Asim
(
Harlingen Medical Center
, Harlingen , Texas , United States )
George, Augustine
(
STHS-McAllen
, Pharr , Texas , United States )
Hassan, Hafeez
(
Adena Regional Medical Center
, Grove city , Ohio , United States )
Koshy, Santhosh
(
Western Michigan University
, Kalamazoo , Michigan , United States )