Risk of Incident Chronic Kidney Disease Among Subtypes of Prevalent and Incident Cardiovascular Disease: UK Biobank
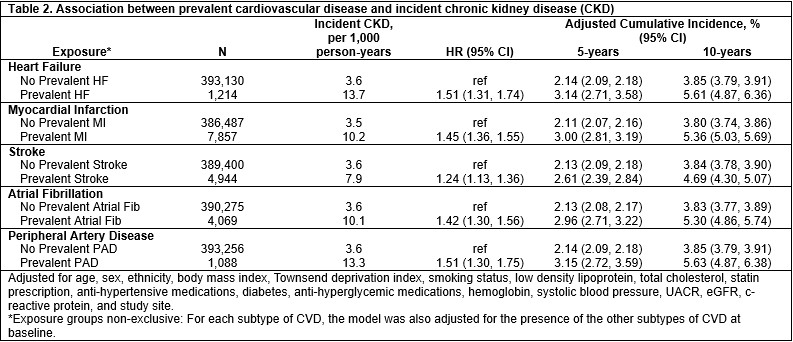
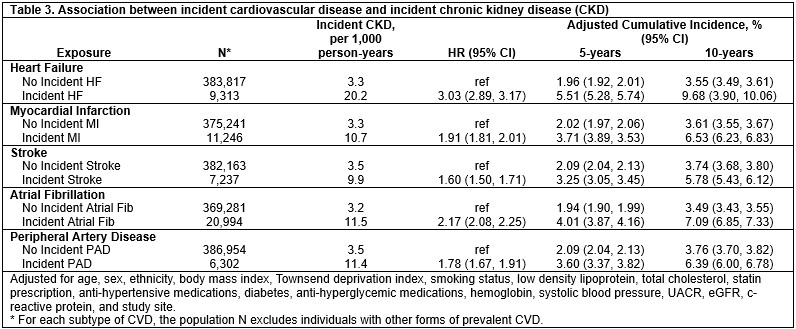
Abstract Body: Introduction: Cardiovascular disease (CVD) and chronic kidney disease (CKD) are interconnected through shared risk factors and vascular pathology. CKD is a well-established driver of cardiovascular morbidity and mortality, but risk for the development of new-onset CKD after CVD remains poorly defined. Current CVD guidelines lack recommendations for kidney function or albuminuria screening and thus it is rarely performed in clinical settings. We aimed to estimate the risk of incident CKD among individuals with subtypes of prevalent CVD and following incident CVD events. Methods: We analyzed 394,344 participants from the UK Biobank, excluding individuals with baseline CKD (estimated glomerular filtration rate <60mL/min/1.73m2 or urine albumin-to-creatinine ratio >30mg/g). Participants were stratified by prevalent CVD subtype—heart failure (HF), myocardial infarction, stroke, atrial fibrillation, or peripheral artery disease (PAD)—using diagnostic codes. Multivariable Cox regression models estimated hazard ratios (HR) for incident CKD adjusting for demographics, socioeconomic status, comorbidities, laboratory values, medications, and study site. Adjusted 5- and 10-year cumulative CKD incidences were derived from the models. Analyses were repeated for incident CKD following incident CVD events. Results: The sample was 54.4% female with mean age 56.7 years. Over a median follow-up of 13.5 years, all subtypes of prevalent CVD were independently associated with increased risk of incident CKD. Incidence rates were highest for HF (10.6/1000 person years) and PAD (12.4/1000 person years), in the absence of other CVD. Participants with HF and PAD had the highest relative and absolute risks for incident CKD compared to no CVD (HF: HR 1.51, 95%CI 1.31–1.74; PAD: HR 1.51, 95%CI 1.30–1.75). The 10-year adjusted cumulative CKD incidences were 5.6% (95%CI 4.9–6.4) for HF and 5.3% (95%CI 4.9–5.7) for PAD. The lowest risk was observed for prevalent stroke (HR 1.24, 95%CI 1.13–1.36). Among incident CVD events, incident HF was associated with the highest risk (HR 3.03, 95%CI 2.89–3.17) of subsequent CKD, corresponding to a 10-year adjusted cumulative incidence of 9.7% (95%CI 9.3–10.1). Conclusions: Both prevalent and incident CVD are associated with substantially increased risk of developing CKD. These findings support incorporating CKD screening into post-CVD care pathways, particularly following HF or PAD, to facilitate early identification and prevention of CKD progression.
Claudel, Sophie
(
Boston Medical Center
, Boston , Massachusetts , United States )
Zhao, Runqi
(
Boston University
, Boston , Massachusetts , United States )
Schmidt, Insa
(
Boston Medical Center
, Boston , Massachusetts , United States )
Srivastava, Anand
(
University of Illinois Chicago
, Chicago , Illinois , United States )
Lloyd-jones, Donald
(
Boston University Medical Center
, Boston , Massachusetts , United States )
Waikar, Sushrut
(
Boston University
, Boston , Massachusetts , United States )
Verma, Ashish
(
Boston University
, Boston , Massachusetts , United States )