EPI-Lifestyle Scientific Sessions 2026
/
Poster Session 3
/
Joint Impact of Social Determinants of Health Burden and Coronary Artery Disease on All-Cause and Cardiovascular Mortality: 18-Year Follow-up From National Health And Nutrition Examination Survey 2000–2018
American Heart Association
57
0
Final ID: TH902
Joint Impact of Social Determinants of Health Burden and Coronary Artery Disease on All-Cause and Cardiovascular Mortality: 18-Year Follow-up From National Health And Nutrition Examination Survey 2000–2018
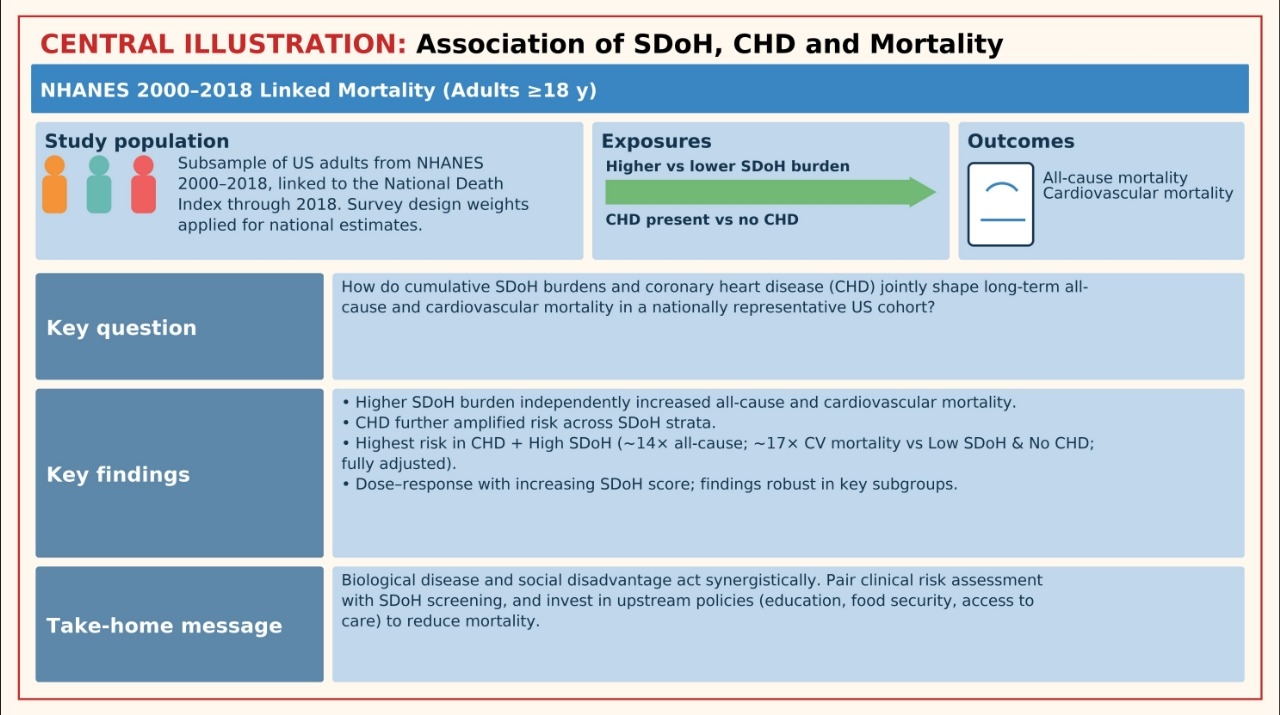
Abstract Body: Background Coronary heart disease (CHD) remains the leading cause of death in the United States, yet the benefits of modern cardiovascular care are not equitably distributed. Social determinants of health (SDoH), which includes economic stability, education, healthcare access, and neighborhood environment, may substantially shape outcomes among patients with CHD. Our study evaluates the joint association of SDoH burden and CHD with mortality outcomes.
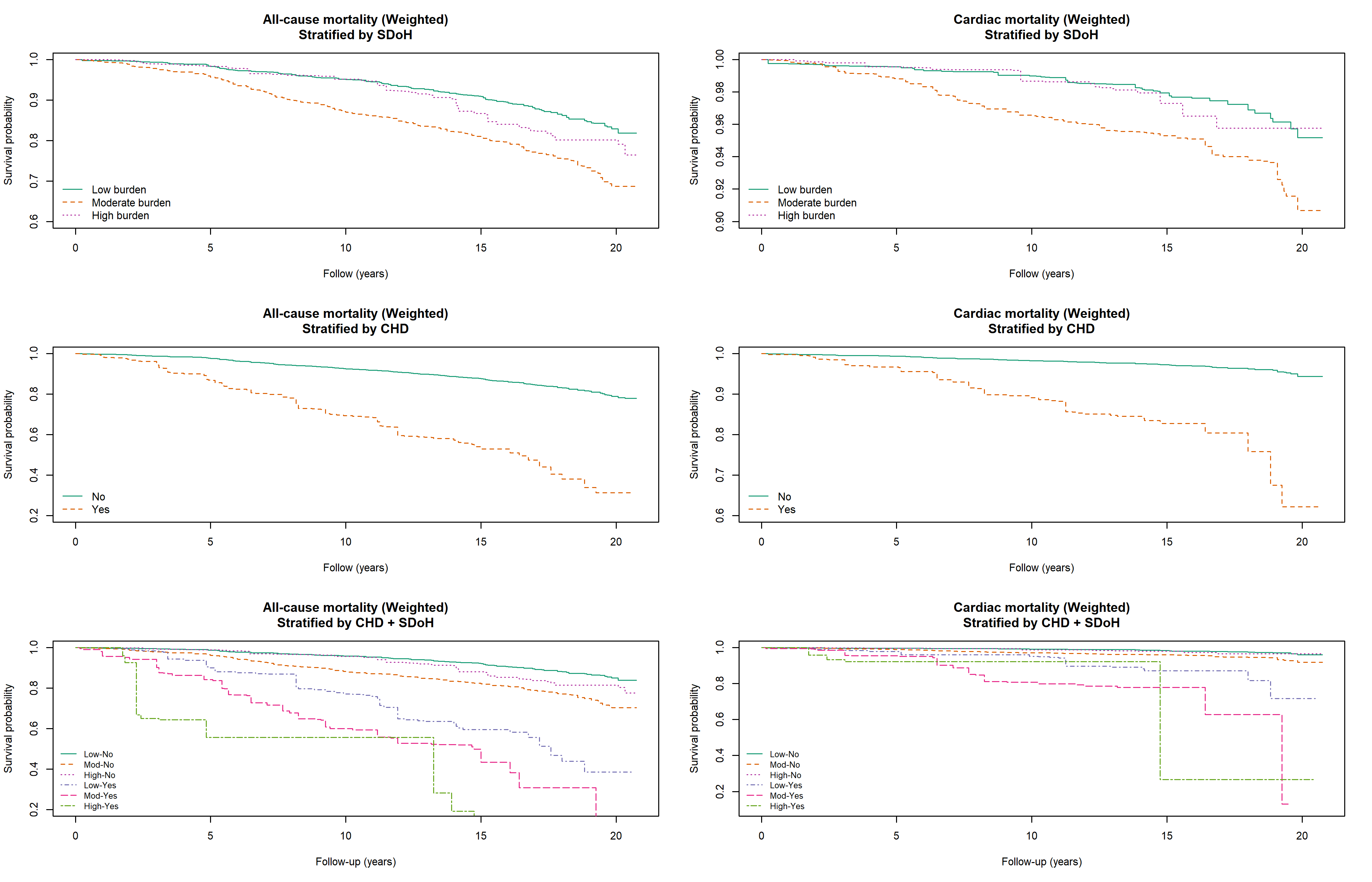
Methods We analyzed adults ≥20 years from the National Health and Nutrition Examination Survey (NHANES) 2000–2018, linked with the National Death Index through 2018. Cumulative SDoH burden was derived from eight domains (employment, poverty-to-income ratio, food insecurity, education, healthcare access, insurance, housing, marital status), categorized as low (0–2), moderate (3–5), or high (6–8). Weighted Cox proportional hazards models estimated hazard ratios (HRs) and 95% confidence intervals (CIs) for all-cause and cardiovascular mortality by SDoH burden, stratified by CHD status, with sequential adjustment for demographic and cardiometabolic factors.
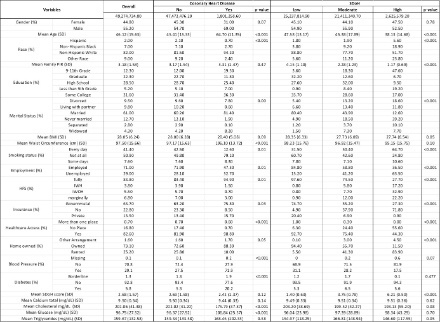
Results Among 49.3 million U.S. adults (mean age 46.1 ± 15.6 years; 44.8% female), 3.7% had CHD. Those with CHD were older (64.7 vs 45.4 years, p < 0.001), more often non-Hispanic White (94.2% vs 81.5%), and had greater waist circumference (106.1 vs 87.5 cm) but lower cholesterol (176 vs 202 mg/dL, p < 0.001). Participants with high SDoH burden had lower income and education. In weighted regression, higher SDoH burden and CHD were independently associated with greater all-cause and cardiovascular mortality. Fully adjusted models showed high SDoH burden tripled all-cause mortality risk (HR 3.00, p < 0.001), while CHD further amplified risk. Compared with low SDoH/no CHD, those with CHD and high SDoH burden had nearly a 14-fold higher all-cause mortality (HR 13.6, p < 0.001) and 17-fold higher cardiovascular mortality (HR 17.7, p < 0.001). Findings were consistent across sex, race, and metabolic subgroups, with mortality hazards often exceeding tenfold among those with both CHD and high SDoH burden.
Conclusions Cumulative SDoH burden is strongly and independently associated with mortality among adults with CHD, with evidence of a synergistic effect between biological and social vulnerability. These findings underscore the need for policies and interventions addressing upstream social inequities to improve survival in cardiovascular populations.
Nizam, Muhammad
(
Trinity Health Livonia/Wayne State University
, Livonia , Michigan , United States )
Kamel, Omar
(
South valley university
, Sohag , Egypt )
Goel, Anika
(
Kakatiya Medical College, Telangana
, Hyderabad , India )
Sharma, Grishma
(
Mayo Clinic
, Jacksonville , Florida , United States )
Adusumilli, Devika
(
Medical City Fort Worth
, Fort Worth , Texas , United States )
Gohar, Najam
(
Ameer-ud-Din Medical College
, Sialkot , Pakistan )
Ahmed, Faizan
(
Jersey Shore University Medical Center
, Neptune City , New Jersey , United States )
Shahid, Izza
(
Houston Methodist Academic Institut
, Houston , Texas , United States )