Non-Invasive Endotyping in Patients with Angina and No Obstructive Coronary Artery Disease: A Randomized, Controlled Trial
Abstract Body (Do not enter title and authors here): Hypothesis: In patients with suspected angina and no obstructive coronary arteries (ANOCA), a stress cardiovascular magnetic resonance (CMR) imaging strategy changes the diagnosis and improves health status.
Design: A prospective diagnostic study and nested RCT.
Population: 250 patients with possible ANOCA <3-months post-angiography.
Setting: 3 hospitals, UK
Intervention (diagnostic): IV adenosine stress/rest CMR imaging (1.5Tesla)
Randomization (1:1) Intervention group: disclosure of myocardial blood flow (MBF, ml/min/g) to inform the final diagnosis and endotype-directed therapy. Control group: MBF measured and not disclosed (angiography-guided usual care). Participants and clinicians were blind to group and CMR results.
Power: If 6-month SAQ summary score (SAQ-SS) is obtained in 200 patients, the trial will have 80% power to detect a mean between-group difference in SAQ-SS of 0.40 SD units.
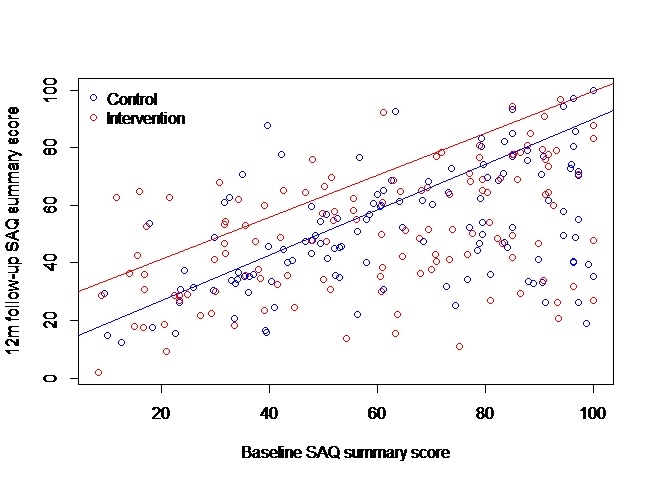
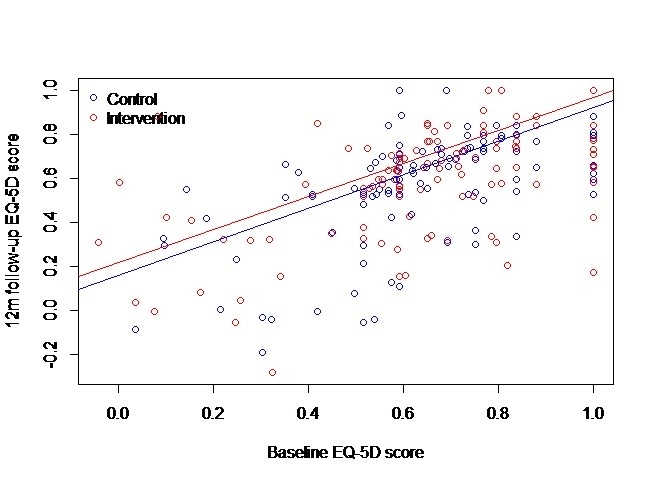
End Points, Primary: The reclassification rate of the initial diagnosis (informed by coronary angiography) vs. the final diagnosis (after CMR). Secondary: SAQ-SS; EQ-5D 5-level; 6- and 12-months.
Results: 273 patients were screened and 250 (91.6%; mean age 63.3 years, 50.4% women) underwent CMR. Post-angiogram, pre-CMR, 243 (97.6%) were diagnosed as non-cardiac chest pain. Post-CMR, the diagnosis was reclassified in 131 (52.4%, 95% CI: 46.0%, 58.7%) participants. Final diagnoses (per participant): 0 (0.0%) obstructive coronary disease, 127 (50.8%) microvascular angina, 119 (47.6%) non-cardiac chest pain, and 4 (1.6%) other diagnoses.
250 patients were randomized and followed for 12 months. In the intervention arm, 61 (49.2%) had a final diagnosis of microvascular angina, a difference of 48.4% (95% CI: 38.7%, 58.1%). Non-cardiac chest pain was predominant in the control arm (96.7%) and reduced in the intervention arm (48.4%). At six months, the mean±SD SAQ-SS in the intervention and control groups were 67.3±21.7 (18.1±19.0 Δ baseline) vs. 53.7±23.4 (0.7±19.8 Δ baseline) (adjusted mean difference: 15.6 (11.1, 20.2; p<0.001) and these differences were evident at 12 months (70.9±23.6 (21.7±22.6 Δ baseline) vs. (52.1±24.1, -0.8 (20.4) Δ baseline (adjusted mean difference: 20.9 (15.8, 26.0)). EQ-5D-5L improved in the intervention group (adjusted mean difference) at 6 months (0.050 (0.004, 0.096)) and 12 months: 0.088 (0.043, 0.134)).
Conclusions: In patients with possible ANOCA, a CMR strategy commonly reclassified the diagnosis and improved angina and health-related quality of life.
Berry, Colin
(
University of Glasgow
, Glasgow , United Kingdom )
Bradley, Conor
(
University of Glasgow
, Glasgow , United Kingdom )
Mckinley, Gemma
(
University of Glasgow
, Glasgow , United Kingdom )
Stanley, Bethany
(
University of Glasgow
, Glasgow , United Kingdom )
Tiller, Christina
(
Innsbruck Medical University
, Innsbruck , Austria )
Ang, Daniel
(
University of Glasgow
, Glasgow , United Kingdom )
Morrow, Andrew
(
University of Glasgow
, Glasgow , United Kingdom )
Sykes, Robert
(
University of Glasgow
, Glasgow , United Kingdom )
Mcgeoch, Ross
(
University Hospital Hairmyres
, East Kilbride , United Kingdom )
Carrick, David
(
University Hospital Hairmyres
, East Kilbride , United Kingdom )
Kellman, Peter
(
NIH
, BETHESDA , Maryland , United States )
Good, Richard
(
Golden Jubilee National Hospital
, Clydebank , United Kingdom )
Mcconnachie, Alex
(
University of Glasgow
, Glasgow , United Kingdom )
Author Disclosures:
Colin Berry:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Abbott:Active (exists now)
; Research Funding (PI or named investigator):Zoll Medical:Active (exists now)
; Research Funding (PI or named investigator):Xylocor :Active (exists now)
; Advisor:Novartis:Past (completed)
; Advisor:Servier:Past (completed)
; Advisor:Merck:Active (exists now)
; Advisor:Edwards LifeSciences:Active (exists now)
; Researcher:CorFlow:Active (exists now)
; Research Funding (PI or named investigator):Boehringer Ingelheim:Active (exists now)
; Research Funding (PI or named investigator):AstraZeneca:Past (completed)
; Advisor:AskBio:Active (exists now)
| David Carrick:DO NOT have relevant financial relationships
| Peter Kellman:No Answer
| Richard Good:No Answer
| Alex McConnachie:DO NOT have relevant financial relationships
| Conor Bradley:DO NOT have relevant financial relationships
| Gemma McKinley:DO NOT have relevant financial relationships
| Bethany Stanley:DO NOT have relevant financial relationships
| Christina Tiller:No Answer
| Daniel Ang:DO NOT have relevant financial relationships
| Andrew Morrow:No Answer
| Robert Sykes:DO have relevant financial relationships
;
Independent Contractor:Novartis:Past (completed)
; Research Funding (PI or named investigator):Medical Research Council:Active (exists now)
| Ross McGeoch:No Answer