Cost-Effectiveness of AI-Enabled Coronary Plaque Analysis for Management of Stable Coronary Artery Disease
Abstract Body (Do not enter title and authors here): Introduction: Recent clinical studies have established that non-calcified plaque in the coronary arteries plays a greater role in risk of myocardial infarction (MI) than calcified plaque. AI-enabled coronary plaque analysis (AI-CPA) derived from coronary computed tomography angiography (CCTA) measures non-calcified plaque in addition to calcified plaque to help guide medical management. The cost-effectiveness of AI-CPA has not been established.
Methods: We developed a Markov cohort model to determine the cost-effectiveness of AI-CPA (Heartflow Inc.) compared to CCTA-only based on data from the FISH&CHIPS study, which consisted of patients undergoing CCTA for suspected stable coronary artery disease (CAD). Total Plaque Volume (TPV) was measured using AI-CPA and divided into stages: 1-100, 101-250, 251-750, >750mm3. TPV stages were used to guide lipid-lowering therapy (Table 1). Cardiovascular (CV) outcomes included all-cause death and MI. Costs were derived from US claims data. Utilities were derived from peer-reviewed literature. Results were reported as incremental cost effectiveness ratios (ICER) over a 5 and 10-year time horizon. Sensitivity analyses were performed to assess the impact of key variables on the model output.
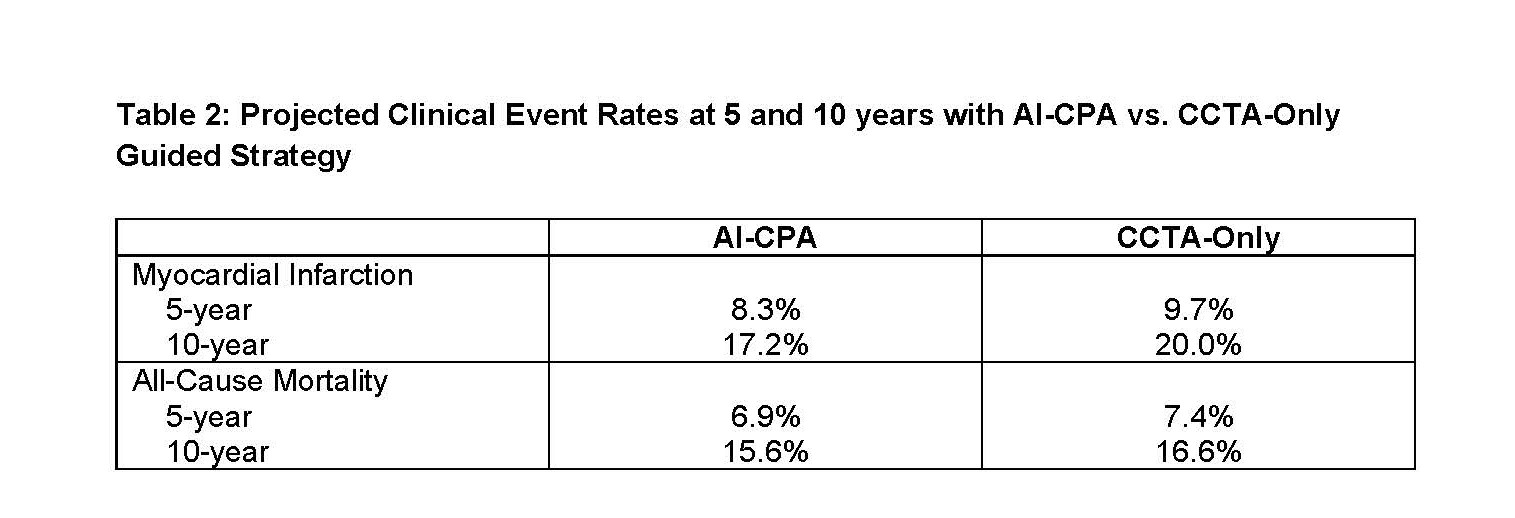
Results: Clinical event rates were projected to be lower with AI-CPA tailored treatment at both 5 years and 10 years (Table 2). AI-CPA patients accrued an average of 0.19 (95% CI: 0.15 to 0.24) and 0.61 QALY (95% CI:0.47 to 0.76) relative to CCTA-only at 5 and 10 years, respectively. Estimated total costs were higher for AI-CPA relative to CCTA-only by $1,519 (95% CI: $1,109 to $1,896) and $1,698 (95% CI: $901 to $2503) at 5 and 10 years, respectively. The ICER at 5 and 10 years was $7,982/QALY and $2,765/QALY, respectively. 100% of the Monte Carlo simulated ICERs were <$100,000/QALY for both time horizons. costs was $17,519 (95% CI: $12,951 to $22,879) and $59,653 (95% CI: $46,358 to $75,690) higher for AI-CPA than CCTA-only at 5 and 10 years, respectively.
Conclusion: An AI-CPA guided approach to medical management of stable CAD may be cost-effective compared to CCTA-only over time due to a reduction in CV events.
Baron, Suzanne
(
Massachusetts General Hospital
, Boston , Massachusetts , United States )
Rogers, Campbell
(
HeartFlow
, Westwood , California , United States )
D'attilio, Daniel
(
HeartFlow
, Westwood , California , United States )
Sengupta, Souma
(
HeartFlow Inc
, Mountain View , California , United States )
Fairbairn, Timothy
(
Liverpool Heart and Chest Hospital
, Lymm , United Kingdom )
Author Disclosures:
Suzanne Baron:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Boston Scientific Corp:Active (exists now)
; Advisor:Edwards LifeSciences:Active (exists now)
; Advisor:Abbott:Active (exists now)
; Advisor:Recor Medical:Active (exists now)
; Research Funding (PI or named investigator):Acarix:Active (exists now)
; Consultant:Janssen:Active (exists now)
; Advisor:Zoll medical:Active (exists now)
; Speaker:Zoll Medical:Active (exists now)
; Consultant:Chiesi:Active (exists now)
; Consultant:Picardia:Active (exists now)
; Speaker:Medtronic:Active (exists now)
; Advisor:Medtronic:Active (exists now)
; Research Funding (PI or named investigator):Abiomed:Active (exists now)
; Advisor:Boston Scientific Corp:Active (exists now)
| Campbell Rogers:DO have relevant financial relationships
;
Employee:Heartflow:Active (exists now)
; Individual Stocks/Stock Options:Heartflow:Active (exists now)
; Executive Role:Heartflow:Active (exists now)
| Daniel D'Attilio:DO NOT have relevant financial relationships
| Souma Sengupta:DO have relevant financial relationships
;
Employee:Heartflow:Active (exists now)
| timothy fairbairn:DO NOT have relevant financial relationships