Association of Inhaled Nitric Oxide with VA-ECMO Weaning and Short-Term Outcomes in ECPELLA Patients: A Retrospective Study
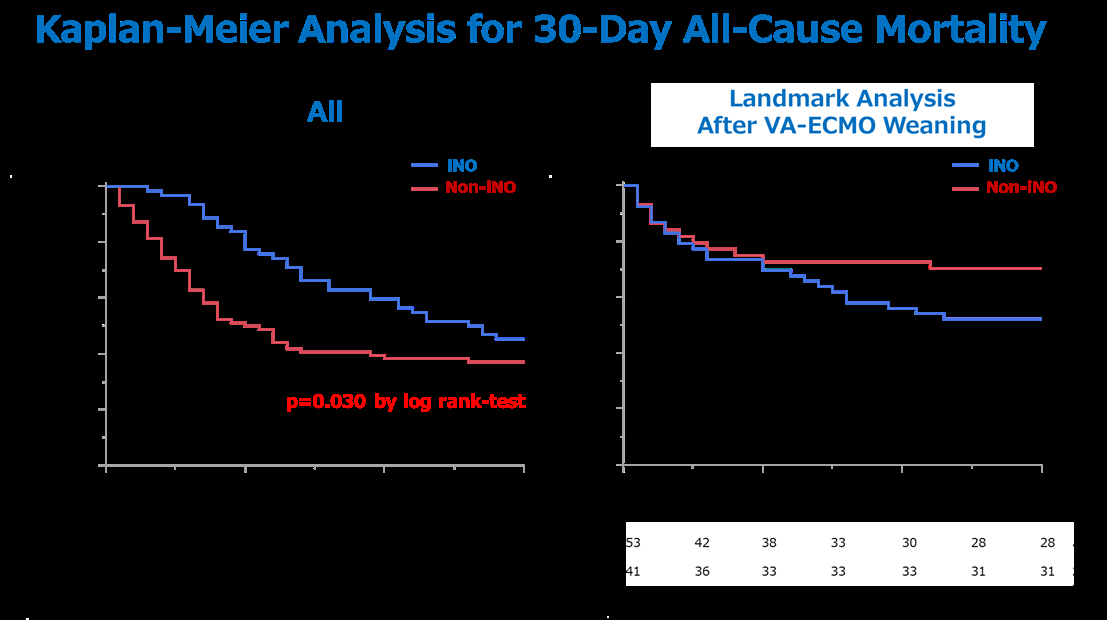
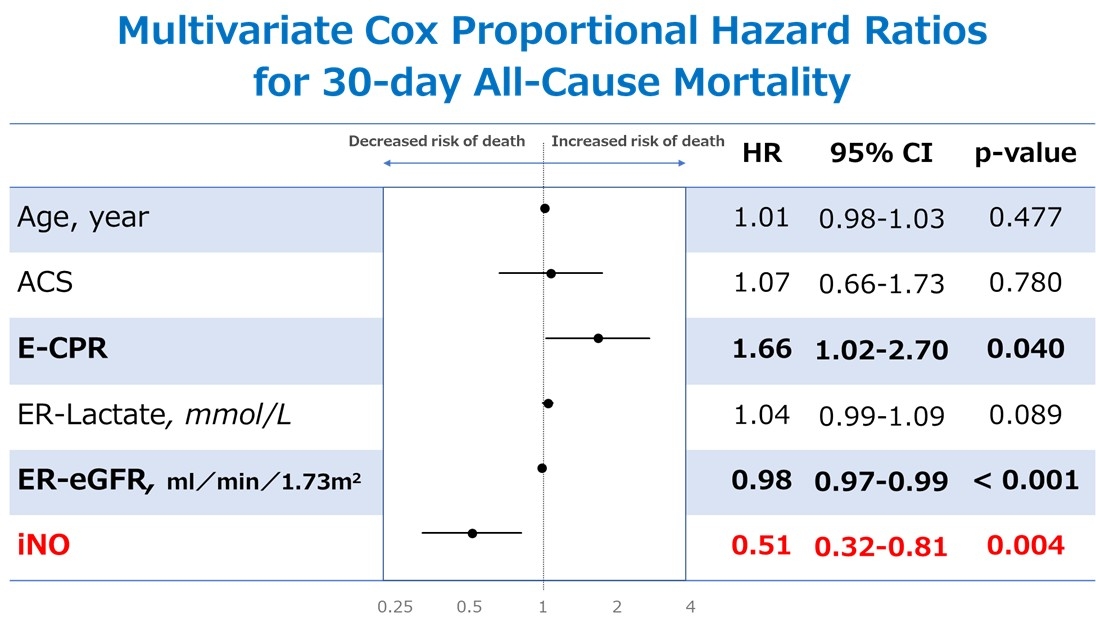
Abstract Body (Do not enter title and authors here): Background: Veno-arterial extracorporeal membrane oxygenation (VA-ECMO) combined with the Impella left ventricular assist device (ECPELLA) has emerged as a promising strategy for cardiogenic shock. Inhaled nitric oxide (iNO) selectively reduces pulmonary vascular resistance, thereby lowering right ventricular afterload and improving right ventricular function. These effects suggest iNO may be beneficial during VA-ECMO weaning in ECPELLA patients. Research Question: This single-center retrospective study evaluated whether iNO therapy in ECPELLA patients was associated with VA-ECMO weaning and short-term outcomes. Methods: Between October 2018 and May 2025, 151 patients received ECPELLA support at our institution. Since 2022, iNO has been available and administered at the discretion of the attending physician. Primary outcomes were 30-day all-cause mortality, VA-ECMO weaning rate, and VA-ECMO duration. Secondary outcomes included changes in hemodynamic parameters and mechanical circulatory support flow, evaluated before and 24 hours after iNO initiation in the iNO group. Results: Of 151 patients, 64 received iNO therapy and 87 did not. There were no significant differences in age, sex, comorbidities, acute coronary syndrome, extracorporeal cardiopulmonary resuscitation (E-CPR), or initial lactate levels. Renal impairment was more prevalent in the iNO group. In that group, VA-ECMO flow significantly decreased 24 hours after iNO initiation, while pulmonary artery pressure, pulmonary artery pulsatility index, cardiac output, and Impella flow remained unchanged. The iNO group had a significantly higher VA-ECMO weaning rate (86% vs. 51%, p < 0.001) and longer VA-ECMO duration (6.3 [4.7–9.8] vs. 4.1 [2.0–6.2] days, p < 0.001). Kaplan–Meier analysis showed improved 30-day survival in the iNO group (45% vs. 38%, p = 0.030). Multivariate Cox analysis revealed E-CPR (HR: 1.66, 95% CI: 1.02–2.70, p = 0.040), eGFR (HR: 0.98, 95% CI: 0.97–0.99, p < 0.001), and iNO use (HR: 0.51, 95% CI: 0.32–0.81, p = 0.004) were significantly associated with 30-day mortality. Conclusion: In ECPELLA-supported patients, iNO was associated with higher VA-ECMO weaning rate and improved 30-day survival despite longer VA-ECMO duration. Prospective studies are needed to identify those who benefit most from iNO.
Tanaka, Motomaro
(
Saiseikai Kumamoto Hospital
, Kumamoto City , Japan )
Unoki, Takashi
(
SAISEIKAI KUMAMOTO HOSPITAL
, Kumamoto City , Japan )