Impact of ECPELLA on Mid-Term Survival and Neurological Outcomes in Patients with Refractory Cardiac Arrest Who Received E-CPR
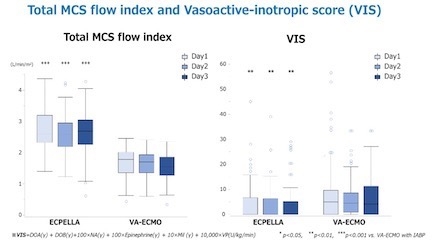
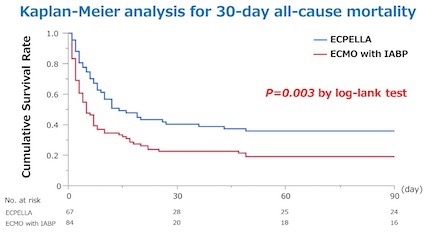
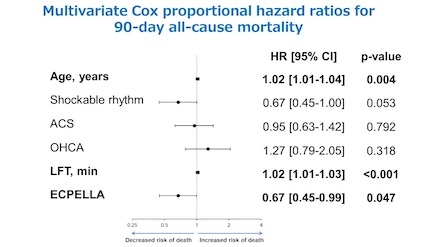
Abstract Body (Do not enter title and authors here): Background: Extracorporeal cardiopulmonary resuscitation (E-CPR) with veno-arterial extracorporeal membrane oxygenation (VA-ECMO) is used for cardiac arrest patients when conventional CPR is ineffective. While VA-ECMO sustains systemic perfusion, it also increases left ventricular (LV) afterload. The recent introduction of the transcatheter LV assist device, Impella, suggests benefits from its combination with VA-ECMO (ECPELLA), but the effectiveness of ECPELLA in E-CPR is still under investigation. Objective: This single-site cohort study aimed to evaluate the impact of ECPELLA versus VA-ECMO combined with intra-aortic balloon pump (IABP) in patients undergoing E-CPR. Method: We performed a retrospective review of 212 consecutive patients who underwent E-CPR at our institute from January 2012 to December 2023. After excluding 61 patients who received VA-ECMO alone, 151 patients were included in the study. These patients were divided into two groups: 67 in the ECPELLA group and 84 in the VA-ECMO with IABP group. We assessed the 90-day survival rate and favorable neurological outcomes, defined as a Cerebral Performance Categories (CPC) score of 1 or 2. Results: No significant differences were noted between the two groups regarding age, male ratio, coronary risk factors, initial shockable rhythm, acute coronary syndrome (ACS), out-of-hospital cardiac arrest (OHCA), and initial lactate levels. The ECPELLA group exhibited a significantly shorter time from cardiac arrest to VA-ECMO placement, known as low flow time (LFT) (35 min [IQR: 18-56] vs. 48 min [IQR: 24-73]; P=0.01), higher total MCS flow, and reduced catecholamine use during the first 72 hours, compared to the VA-ECMO with IABP group. Survival rates and favorable neurological outcomes at hospital discharge were significantly higher in the ECPELLA group (39% vs. 17%, P=0.002; 27% vs. 12%, P=0.02, respectively). The 90-day all-cause mortality was significantly lower in the ECPELLA group (P=0.003 by log-rank test). Multivariate Cox proportional hazard analysis, including age, shockable rhythm, ACS, OHCA, LFT, and ECPELLA, indicated that age (hazard ratio [HR] 1.02, 95% CI 1.01-1.04, P=0.004), LFT (HR 1.02, 95% CI 1.01-1.03, P<0.001), and ECPELLA (HR 0.67, 95% CI 0.45-0.99, P=0.046) were significantly associated with 90-day all-cause mortality. Conclusion: ECPELLA was associated with improved 90-day mortality rates and neurological outcomes in patients who received E-CPR.