Association of Finerenone Use With Cardiovascular and Renal Outcomes in Patients With HFpEF and CKD: A Propensity-Matched Real-World Comparative Effectiveness Study
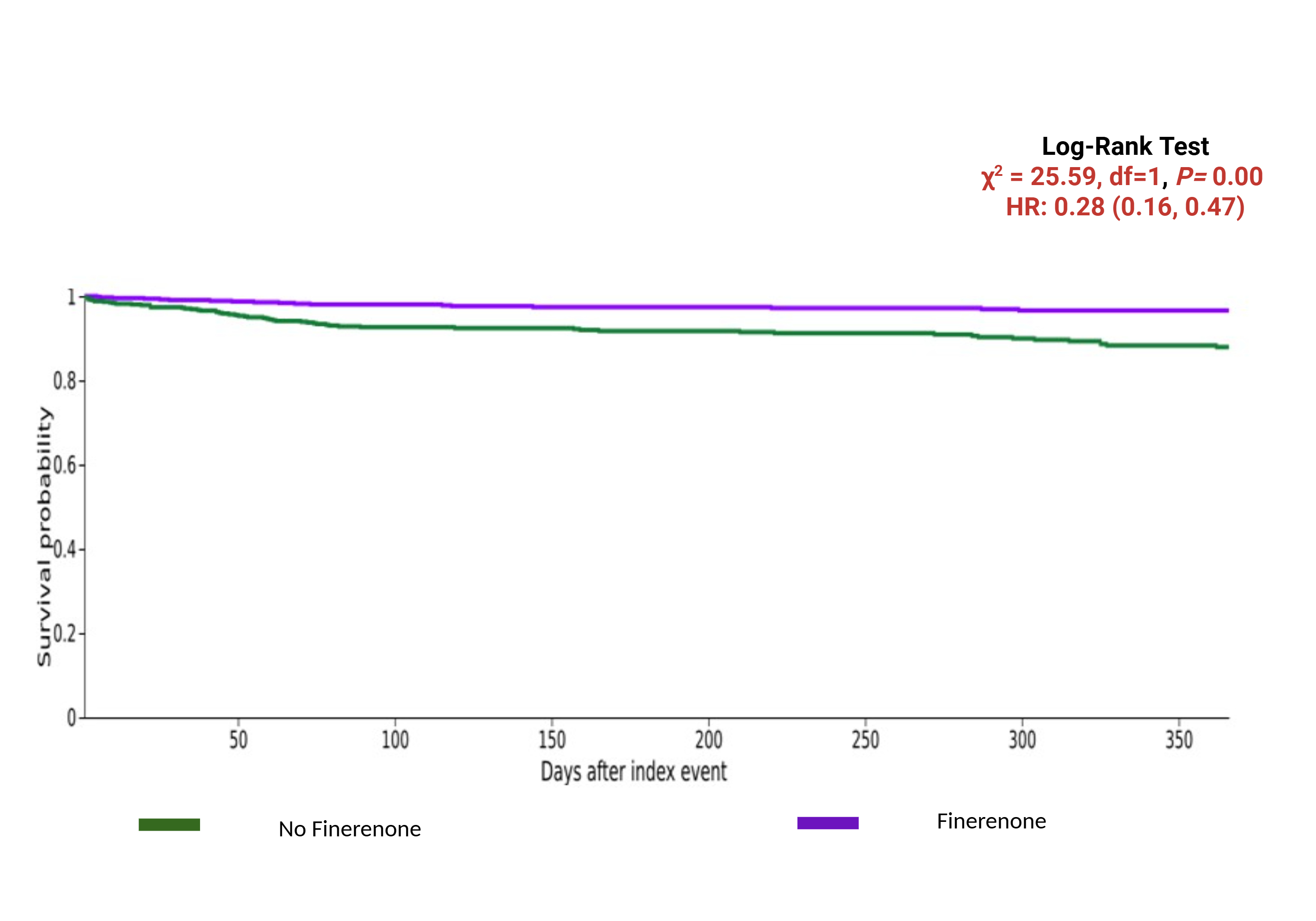
Abstract Body (Do not enter title and authors here): Background: Heart failure with preserved ejection fraction (HFpEF) complicated by chronic kidney disease (CKD) represents a high-risk phenotype with limited therapeutic options. Finerenone, a nonsteroidal mineralocorticoid receptor antagonist, has shown promise in reducing cardiorenal events in CKD, but its role in HFpEF has not been well established. Objective: This study aimed to assess the efficacy of finerenone on all-cause mortality, cardiovascular outcomes, and renal function in patients with HFpEF and CKD using real-world data. Methods: This retrospective cohort study utilized the TriNetX Global Collaborative Network comprising 148 healthcare organizations. Adults (≥18 years) with HFpEF and CKD were identified from July, 2021 till date and divided into two groups, one of them were treated with finerenone and control group with those not treated with finerenone. 1:1 propensity score matching was done on baseline variables including age, gender, race, types of medication, and comorbidity. Both the cohorts were followed for one year. Primary outcome was all-cause mortality (ACM), while secondary outcomes were heart failure exacerbations (HFE), major adverse cardiovascular events (MACE), and cardiovascular death. Safety endpoints including risk of acute kidney injury (AKI), and hypotension were analyzed. Risk ratio (RR) were used to compare outcomes at a follow up of 1 year. Results: After 1:1 PSM, the study cohort comprised 695 patients in both groups. The study population had a mean age of 72 years. PSM analysis at 1 year follow up showed that Finerenone use was associated with significantly lower risk of ACM (RR, 0.29(0.178-0.50); p<0.001), HFE (RR, 0.45(95%CI: 0.27-0.76), p<0.01), CVM (RR, 0.94(95%CI: 0.90-0.99), p=0.01) when compared with control group. However, no significant differences were observed for MACE (RR, 1.32(95%CI: 0.62-2.79), p=0.46), atrial fibrillation/flutter (RR, 0.59(95%CI: 0.28-1.23), p=0.15), ventricular tachycardia (RR, 0.97(95%CI: 0.40-2.31), p=0.94), and ischemic stroke (RR, 0.95(95%CI: 0.40-2.28), p=0.92). The risk of AKI and hypotension were comparable in both the cohorts. Conclusions: In a real-world, propensity-matched cohort of HFpEF patients with CKD, finerenone use was associated with significantly improved survival and fewer HF-related events without increasing cardiovascular or renal adverse events. These findings support further exploration of finerenone in HFpEF populations beyond its current indications.
Hanif, Muhammad
(
Upstate Medical University
, New York , New York , United States )
Jaiswal, Vikash
(
JCCR Cardiology Research
, Jaunpur , India )
Shrestha, Abhigan
(
Medical Research Hub, Nepal
, Kathmandu , Nepal )
Knohl, Stephen
(
Upstate Medical University
, New York , New York , United States )
Author Disclosures:
Muhammad Hanif:DO NOT have relevant financial relationships
| Vikash Jaiswal:DO NOT have relevant financial relationships
| Abhigan Shrestha:DO NOT have relevant financial relationships
| Stephen Knohl:DO NOT have relevant financial relationships