Long-Term Trends in Ischemic Heart Disease Mortality with Chronic Kidney Disease as a Contributing Cause: A 25-Year Sex-Stratified Analysis Using CDC WONDER
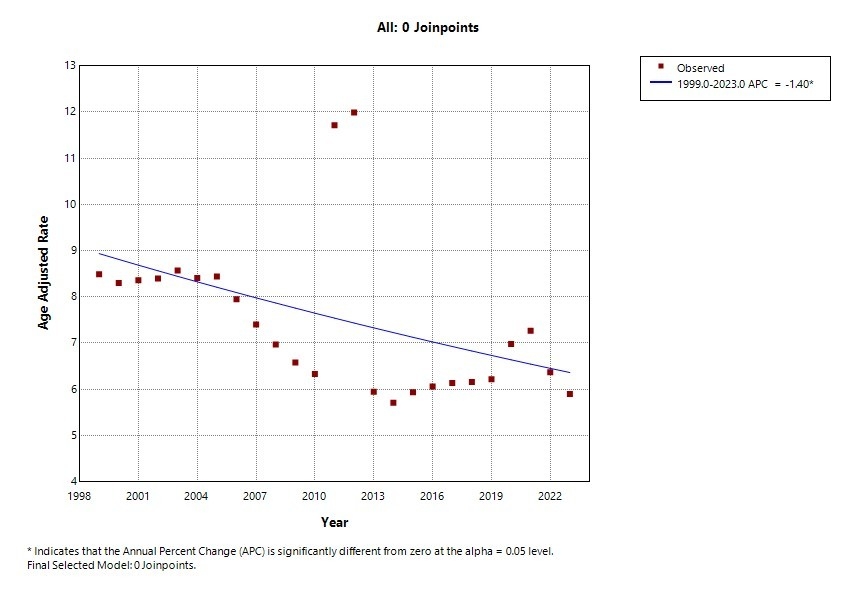
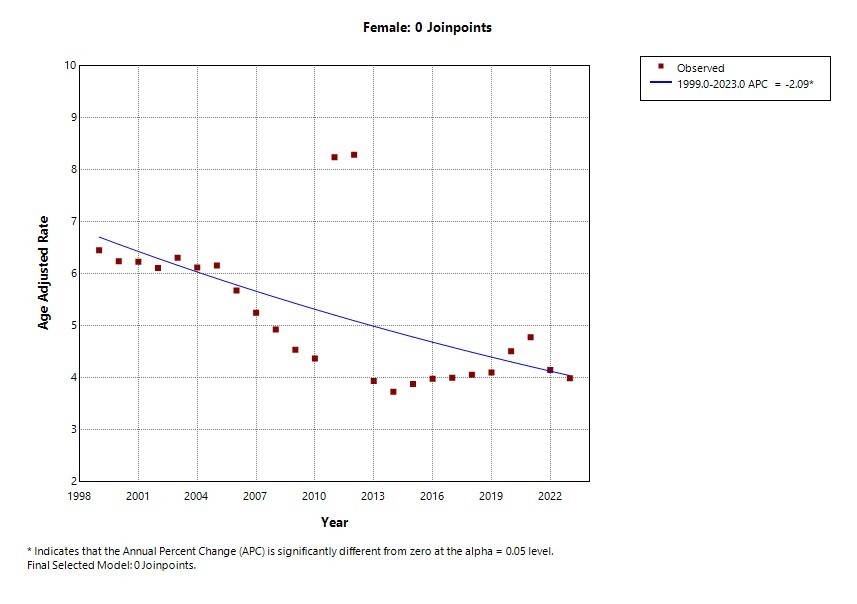
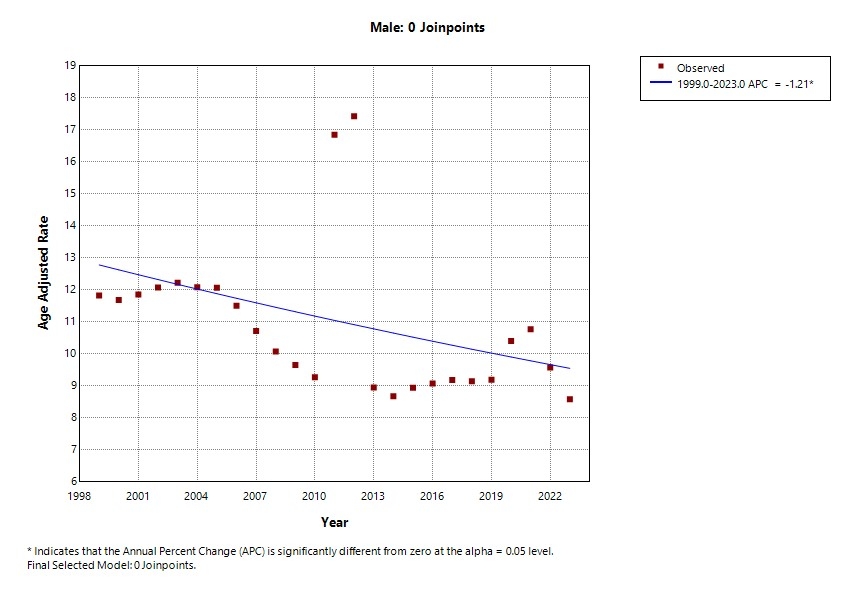
Abstract Body (Do not enter title and authors here): Background: Chronic kidney disease (CKD) is a well-established amplifier of ischemic heart disease (IHD) risk, yet long-term national mortality trends for IHD with CKD as a contributing cause remain underexplored. Given rising CKD prevalence and persistent cardiovascular disparities, understanding sex-specific mortality patterns is critical to inform cardio-renal care and public health strategy. Methods: We extracted U.S. mortality data from the CDC WONDER Multiple Cause of Death database (1999–2023). Cases were included if IHD (ICD-10: I20–I25) was the underlying cause of death and CKD (ICD-10: N18.1–N18.9) was a contributing cause. Age-adjusted mortality rates (AAMRs) per 100,000 population were calculated using the 2000 U.S. standard population. Joinpoint regression analysis identified inflection points and estimated annual percent changes (APCs). Analyses were stratified by sex and overall. Results: Between 1999 and 2023, 633,339 deaths were recorded with IHD as the underlying cause and CKD as a contributing cause. Mortality rates declined significantly across all groups over this 25-year period. Among males, the AAMR decreased from 12.6 to 9.1 per 100,000 (APC −1.21%; p < 0.05) with no joinpoints, indicating a linear decline. In females, AAMRs fell more sharply from 6.5 to 3.9 per 100,000 (APC −2.09%; p < 0.05), also without inflection points. When all sexes were combined, the overall AAMR declined from around 8.9 to 6.1 per 100,000 (APC −1.40%; p < 0.05). No significant inflection points were noted in any of the groups, reinforcing the persistence of a linear, gradually declining mortality trend over the 25-year period. Conclusions: Over the past quarter century, mortality from IHD with CKD as a contributing cause has decreased significantly in the U.S., yet meaningful sex disparities persist. The steeper decline in females may reflect improved access, awareness, or management relative to their male counterparts. These findings highlight the need for renewed emphasis on integrated, sex-sensitive cardio-renal care models. Future interventions should prioritize male populations and emphasize precision strategies to close equity gaps and sustain momentum in cardio-renal mortality reduction.
Sharma, Gaurav
(
JNU Medical College Jaipur
, Jaipur , India )
Pavuluri, Sai Swetha
(
AIIMS, Bhubaneswar
, Bhubaneswar , India )
Sahai, Akshat
(
Texas Tech University Health Sciences Center at the Permian Basin
, Odessa , Texas , United States )
Vashisht, Kumar
(
BronxCare Health System
, New York , New York , United States )
Author Disclosures:
Gaurav Sharma:DO NOT have relevant financial relationships
| Sai Swetha Pavuluri:DO NOT have relevant financial relationships
| Akshat Sahai:DO NOT have relevant financial relationships
| Kumar Vashisht:DO NOT have relevant financial relationships