External Validation of an AI-ECG algorithm for Occlusive Myocardial Infarction Detection in a General Chest Pain Population
Abstract Body (Do not enter title and authors here): Background: Nearly one-third of patients with Acute Coronary Syndrome have an acute coronary occlusion without diagnostic ST elevations (STE) that often goes unrecognized, leading to treatment delays and poorer outcomes. AI-ECG algorithms can identify subtle, clinically under-recognized ECG patterns indicative of occlusive myocardial infarction (OMI). Our team has previously developed a suite of OMI detection AI-ECG models trained on pre-hospital ECGs from multiple sites in the United States. In this study, we externally validate the performance and generalizability of these models in an unselected general chest pain population from the University of Rochester Medical Center (URMC).
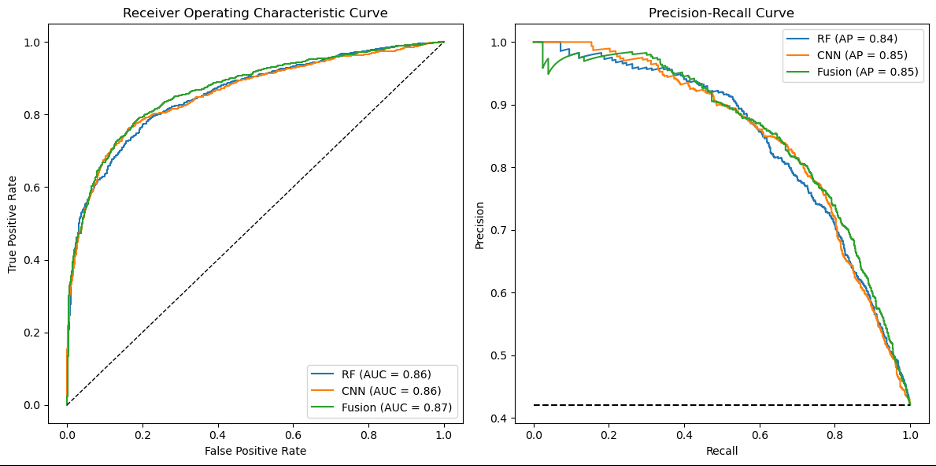
Methods: This was a secondary analysis of ACC Chest Pain-MI Registry at URMC. We included consecutive chest pain patients with available 12-lead ECG data between 2019 and 2023. The ECGs were preprocessed using three previously published AI-ECG models for predicting OMI: a random forest (RF) classifier, a convolutional neural network (CNN), and an RF-CNN fusion model. The primary study outcome was OMI, angiographically defined as coronary stenosis >99% with stent placement or stenosis >70% with stent placement and elevated peak troponin x10 folds. STEMI patients with emergent primary PCI met the primary study outcome. Model performance was evaluated using area under ROC curve (AUC) and average precision (AP). We applied previously identified cutoffs from the derivation cohort for rule-in and rule-out thresholds.
Results: The sample included 2,254 patients (age 63 ± 14; 35% female). Overall, 946 patients (42%) had OMI, of whom 22% did not have STE on presenting ECG. Figures 1 shows the AUC and AP for AI-ECG models. The RF, CNN, and fusion models ruled in 760 (34%), 869 (39%), and 944 (42%) patients at precisions of 0.98, 0.95, and 0.92, respectively. The models ruled out 1494 (66%), 1385 (61%), and 1310 (58%) patients at recall of 0.86, 0.91, and 0.94, respectively. At “high confidence”, the RF-CNN fusion model had the best rule out accuracy, identifying 33% of patients for early discharge with an overall missed events rate of 3.5%. The RF model had the best rule in accuracy, identifying 15% of patients for immediate PCI with overall false CATH lab activation rate of 4%.
Conclusions: Our results demonstrate that our previously developed AI-ECG models for OMI detection generalize well to new unseen data from an external site in the US.
Ji, Rui Qi
(
University of Toronto
, Thornhill , Ontario , Canada )
Riek, Nathan
(
University of Pittsburgh
, Pittsburgh , Pennsylvania , United States )
Dzikowicz, Dillon
(
University of Rochester
, Rochester , New York , United States )
Al-zaiti, Salah
(
UNIVERSITY OF ROCHESTER
, Rochester , New York , United States )
Author Disclosures:
Rui Qi Ji:DO NOT have relevant financial relationships
| Nathan Riek:DO NOT have relevant financial relationships
| Dillon Dzikowicz:DO have relevant financial relationships
;
Advisor:Philips North America:Active (exists now)
| Salah Al-Zaiti:DO NOT have relevant financial relationships