Comparative Effectiveness of Percutaneous Mitral Valve Repair, Surgery, and Medical Therapy in Patients with Mitral Regurgitation: A Network Meta-Analysis
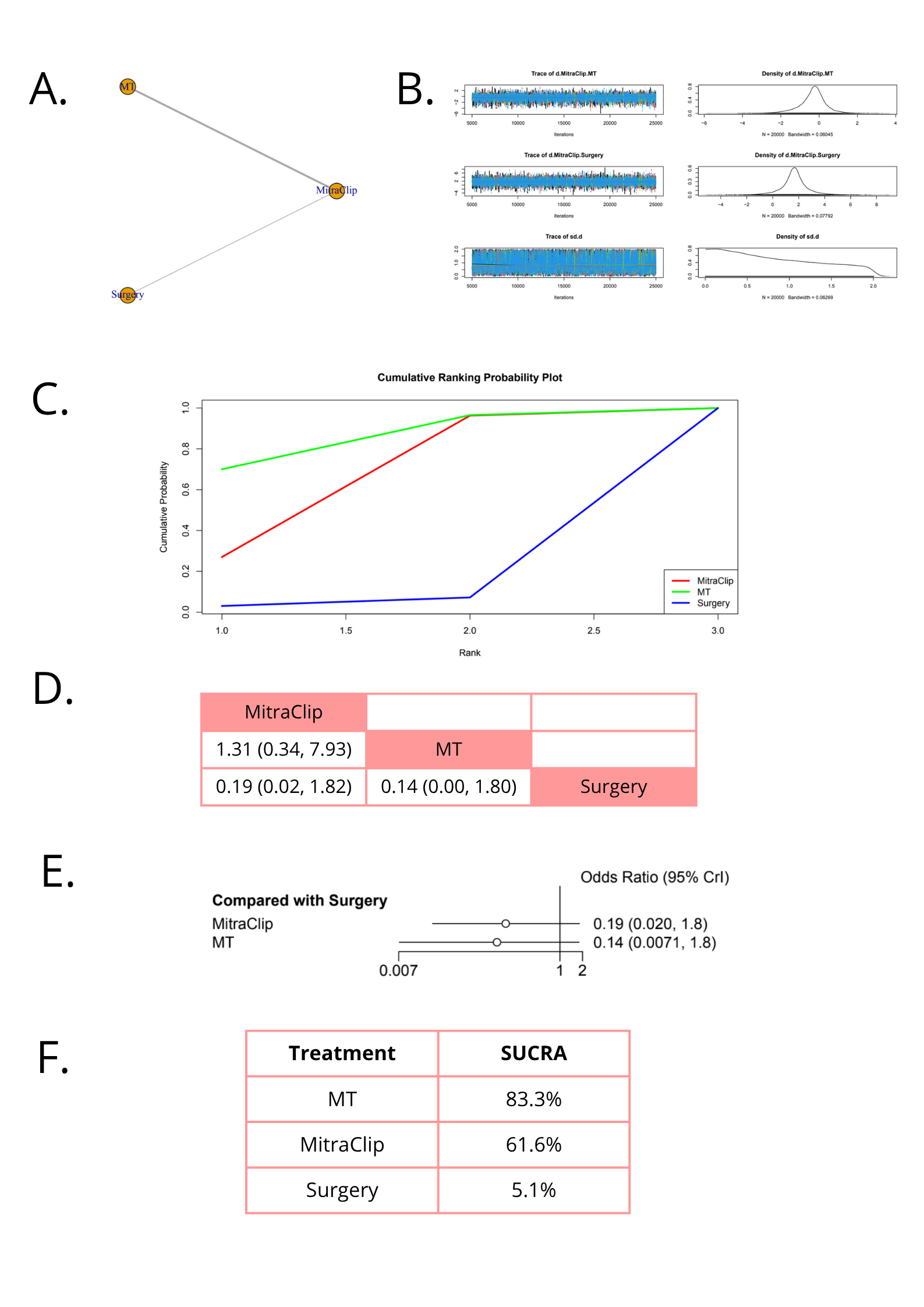
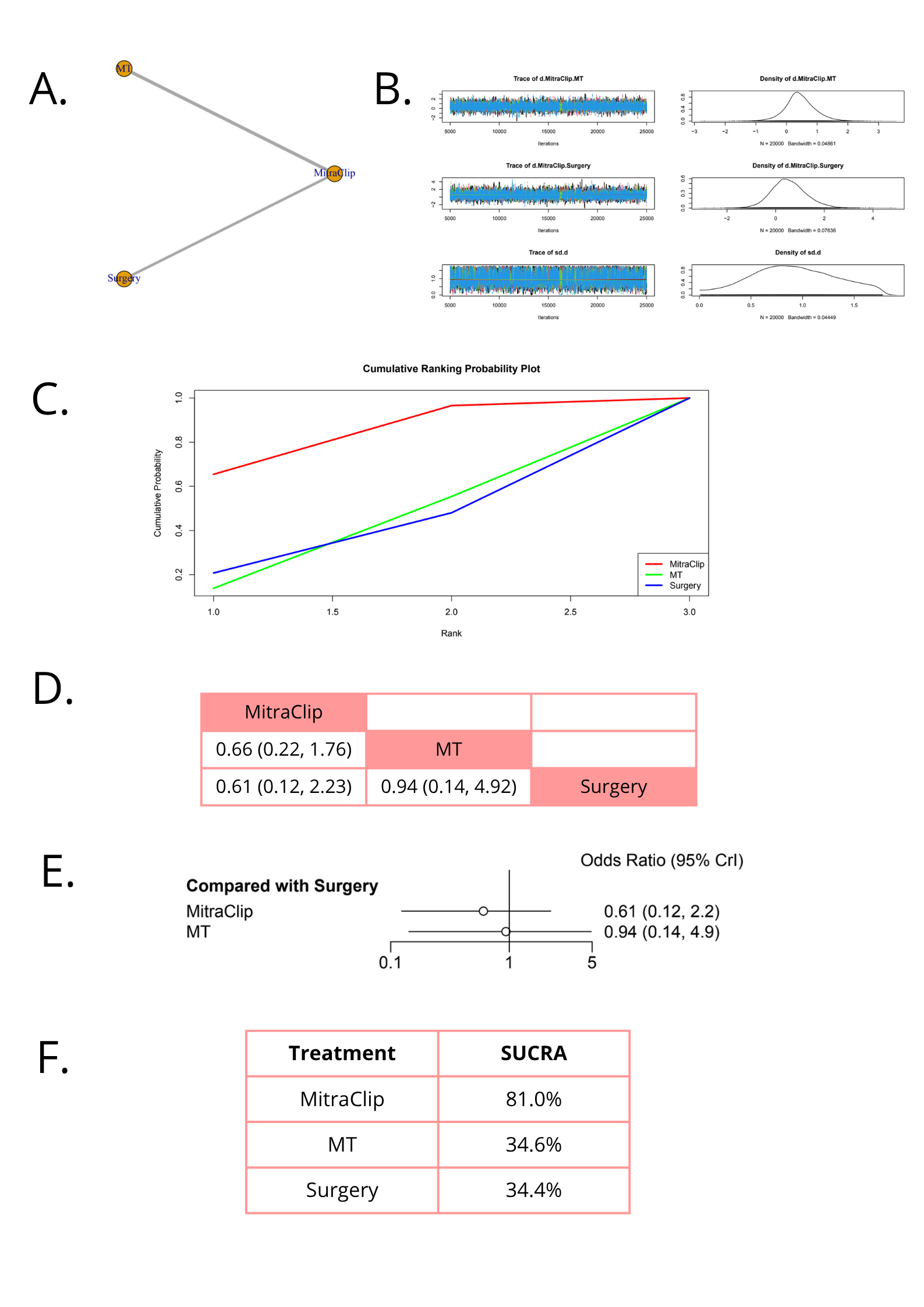
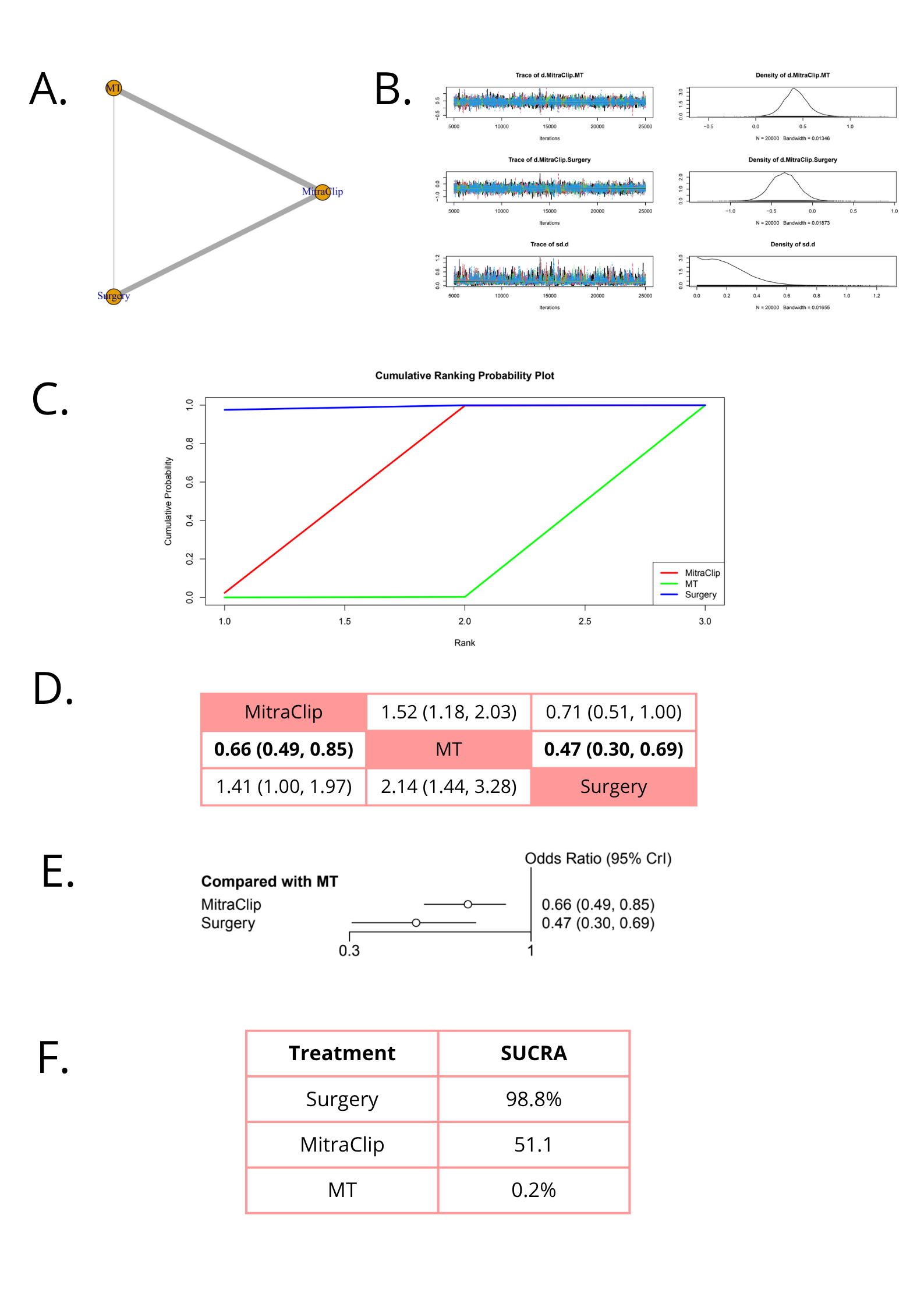
Abstract Body (Do not enter title and authors here): Introduction: Functional mitral regurgitation (MR) is caused by annular dilation or left ventricular remodeling rather than primary valve disease. If untreated, it is linked to adverse outcomes and symptom progression. Percutaneous mitral valve repair (PMVr) with the MitraClip device has emerged as a less invasive alternative to surgery for patients with significant MR, particularly those at high surgical risk. However, the comparative effectiveness of PMVr, surgery, and medical therapy (MT) remains unclear. Methods: We performed a systematic review and network meta-analysis of randomized controlled trials (RCTs) and cohort studies comparing PMVr, surgery, and MT in patients with MR. A comprehensive search of PubMed, Scopus, Cochrane CENTRAL, Embase, and Web of Science was conducted. Data were pooled using a random-effects model. Outcomes included all-cause death (ACD), stroke, serious adverse events, cardiovascular dead (CVD), heart failure rehospitalization, New York Heart Association (NYHA) class I/II, major bleeding, major adverse cardiovascular events (MACE), and myocardial infarction (MI). Results: A total of 20 studies were included, comprising 4,273 patients. The results showed that, compared to surgery, MT was associated with a lower incidence of stroke (OR: 0.10 [0.00–0.61]) and major bleeding (OR: 0.06 [0.01–0.25]). MitraClip was associated with fewer serious adverse events compared to surgery (OR: 0.18 [0.07–0.50]) and showed a potential association with lower CVD (OR: 0.61 [0.12–2.20]). Surgery, when compared to MT, was associated with better NYHA functional class I/II outcomes (OR: 3.2 [1.1–8.6]) and lower ACD (OR: 0.47 [0.30–0.69]). No clear associations were observed for heart failure rehospitalization (OR: 0.46 [0.10–1.80]), MACE (OR: 0.14 [0.00–1.80]), or MI (OR: 0.74 [0.04–10.00]). Conclusion: This network meta-analysis reveals significant differences in the safety and effectiveness of PMVr, surgery, and MT. PMVr may offer a safer profile for high-risk patients. Surgery remains the most effective option for improving function and survival, reinforcing its role as the standard approach in suitable candidates. MT may be reserved for selected cases, but it offers limited long-term benefit. A patient-centered, multidisciplinary strategy is essential to guide treatment choice. Further trials are needed to inform care in intermediate-risk groups.
Gasca, Jose
(
Universidad Santiago de Cali
, Cali , Colombia )
Cueva, Luis E.
(
Universidad Nacional de Piura
, Piura , Peru )
Aragon Cortes, Amiel
(
Universidad Autonoma de Baja Califo
, Tijuana , Mexico )
Torres-chavez, Mario Cesar
(
Facultad de Medicina Mexicali
, Mexicali , Mexico )
Rojas Tellez, Luis Giovanni
(
Universidad Michoacana
, Morelia , Mexico )
Choque Ayala, Luz Camila
(
Universidad Católica Boliviana "San Pablo"
, Santa Cruz de la Sierra , Bolivia, Plurinational State of )
García Loera, Arantza
(
Escuela Superior de Medicina (IPN)
, Ciudad de Mexico , Mexico )
Pech Burgos, Luis Alejandro
(
Universidad Marista
, Merida , Mexico )
Author Disclosures:
Jose Gasca:DO NOT have relevant financial relationships
| Luis E. Cueva:DO NOT have relevant financial relationships
| Amiel Aragon Cortes:DO NOT have relevant financial relationships
| Mario Cesar Torres-Chavez:DO NOT have relevant financial relationships
| Luis Giovanni Rojas Tellez:DO NOT have relevant financial relationships
| Luz Camila Choque Ayala:No Answer
| Adolfo Calderon-Fernandez:DO NOT have relevant financial relationships
| Arantza García Loera:DO NOT have relevant financial relationships
| Luis Alejandro Pech Burgos:DO NOT have relevant financial relationships
Aragon Cortes Amiel, Beltran De La Fuente Andrea Cristina, López Mena Diego, Orozco Santiago Ricardo Alberto, Calderon-fernandez Adolfo, Torrico Beltran Valentina, Cueva Luis E., Natera Dilmareth, Gasca Jose, Zuñiga Montaño Karoly Pamela, Polania Perez Olga Nataly