Post-Discharge Outcomes and Healthcare Costs for Patients Hospitalized for Heart Failure with Transthyretin Amyloid Cardiomyopathy: Findings From GWTG–HF
Abstract Body (Do not enter title and authors here): Background: Transthyretin amyloid cardiomyopathy (ATTR-CM) is associated with high risk for heart failure (HF) hospitalization. However, little is known regarding post-discharge outcomes and healthcare costs for patients with underlying ATTR-CM, as compared with the general HF population.
Methods: We analyzed Medicare beneficiaries hospitalized for HF in the Get With The Guidelines-Heart Failure (GWTG-HF) registry and discharged alive from January 1, 2021, to June 30, 2023. Patients were compared according to the presence or absence of an ATTR-CM diagnosis, as documented in the GWTG-HF case report form. All-cause mortality, HF readmission, and all-cause readmission over 1-year post-discharge were assessed in unadjusted and adjusted risk models. Inpatient, outpatient (excluding medications), and total per-patient healthcare costs over the 1-year post-discharge were calculated from payments made by Medicare.
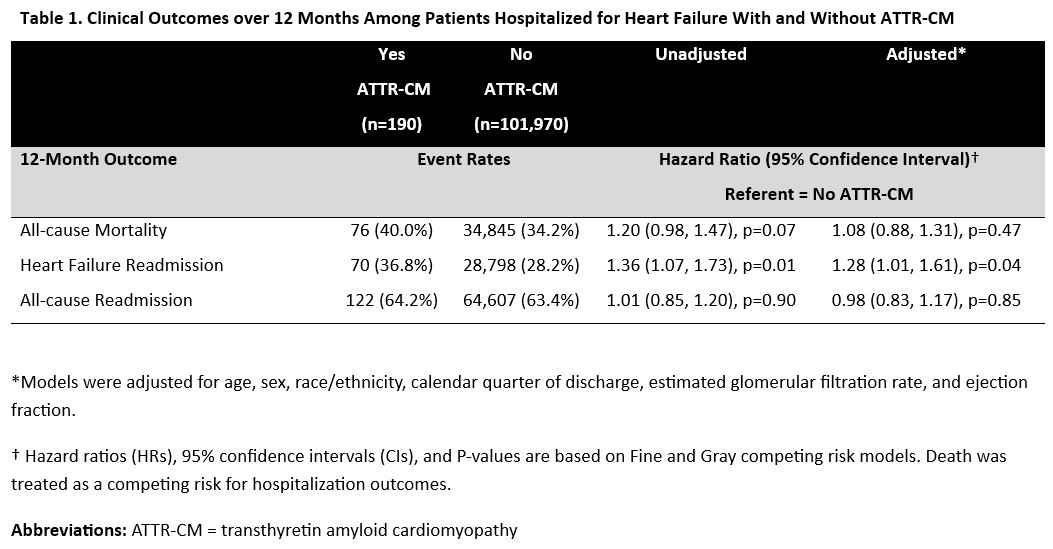
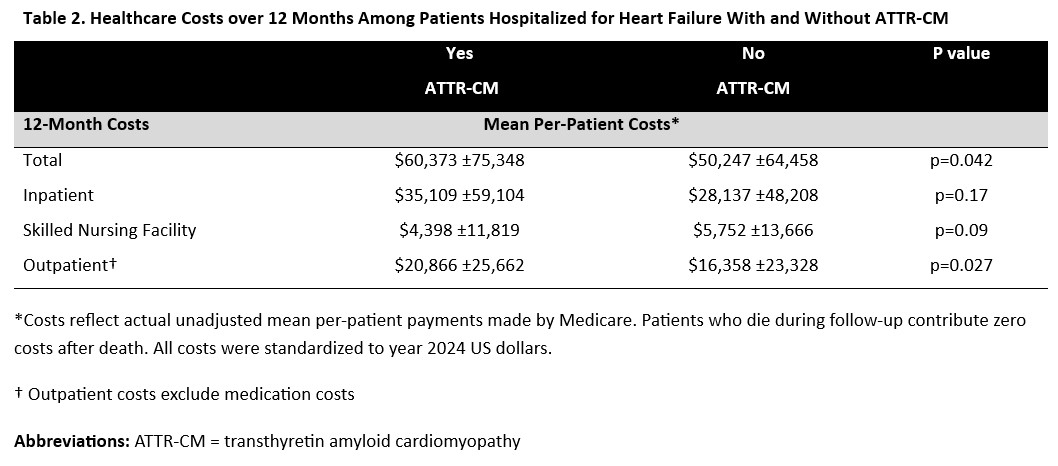
Results: Among 102,160 patients across 563 US hospitals, 190 (0.2%) carried a diagnosis of ATTR-CM. Compared to those without ATTR-CM, patients with an ATTR-CM diagnosis were older (82 [76–87] vs 80 [73–87] years), more likely to be male (68.9% vs 47.0%), and had lower ejection fraction (45 [30–57] vs 53 [35–60]%). Patients with ATTR-CM were significantly more likely to be discharged on a mineralocorticoid receptor antagonist (29.5% vs 20.4%) and SGLT2 inhibitor (21.6% vs 14.1%), and significantly less likely to be discharged on a beta-blocker (52.1% vs 77.6%). After adjustment, ATTR-CM was associated with higher risk of 1-year HF readmission (36.8% vs. 28.2%; HR 1.28, 95% CI 1.01–1.61, p=0.04), but not all-cause mortality (40.0% vs. 34.2%; HR 1.08, 95% CI 0.88–1.31, p=0.47) or all-cause readmission (64.2% vs. 63.4%; HR 0.98, 95% CI 0.83–1.17, p=0.85) (Table 1). Mean 1-year total per-patient Medicare costs were higher among patients with ATTR-CM than those without ($60,373 vs $50,247; p=0.04), primarily driven by significant differences in outpatient costs ($20,866 vs $16,358]; p=0.03) (Table 2).
Conclusion: Among older adults hospitalized for HF in the US, patients with underlying ATTR-CM experience similarly high rates of post-discharge mortality, but face greater risks of HF readmission and accrue higher post-discharge healthcare costs. These findings highlight a disproportionate clinical and economic burden of ATTR-CM compared with the general HF population, further supporting the need for earlier identification and tailored care strategies.
Shoji, Satoshi
(
Duke Clinical Research Institute
, Chapel Hill , North Carolina , United States )
Ikeaba, Uchechukwu
(
Duke Clinical Research Institute
, Durham , North Carolina , United States )
Fonarow, Gregg
(
UCLA MEDICAL CENTER
, Los Angeles , California , United States )
Selvaraj, Senthil
(
Duke University
, Durham , Pennsylvania , United States )
Lewsey, Sabra
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Pandey, Ambarish
(
UT Southwestern Medical Center
, Dallas , Texas , United States )
Khouri, Michel
(
Duke University School of Medicine
, Chapel Hill , North Carolina , United States )
Alhanti, Brooke
(
Duke University
, Durham , North Carolina , United States )
Mcdermott, Jim
(
AstraZeneca / BioPharmaceuticals Medical CVRM
, Wilmiton , Delaware , United States )
Wright, Jason
(
AstraZeneca
, Bryn Mawr , Pennsylvania , United States )
Vaduganathan, Muthiah
(
Brigham and Womens Hospital
, Boston , Massachusetts , United States )
Greene, Stephen
(
Duke Clinical Research Institute
, Durham , North Carolina , United States )
Author Disclosures:
Satoshi Shoji:DO NOT have relevant financial relationships
| Jason Wright:DO have relevant financial relationships
;
Employee:AstraZeneca:Active (exists now)
; Individual Stocks/Stock Options:AstraZeneca:Active (exists now)
| Muthiah Vaduganathan:DO have relevant financial relationships
;
Consultant:American Regent, Amgen, AstraZeneca, Bayer AG, Baxter Healthcare, Bristol Myers Squibb, Boehringer Ingelheim, Chiesi, Cytokinetics, Esperion, Fresenius Medical Care, Idorsia Pharmaceuticals, Lexicon Pharmaceuticals, Merck, Milestone Pharmaceuticals, Novartis, Novo Nordisk, Pharmacosmos, Relypsa, Roche Diagnostics, Sanofi and Tricog Health:Active (exists now)
; Research Funding (PI or named investigator):Amgen, AstraZeneca, Boehringer Ingelheim, Galmed, Novartis, Bayer AG, Occlutech, Pharmacosmos, and Impulse Dynamics:Active (exists now)
| Stephen Greene:DO have relevant financial relationships
;
Consultant:Amgen:Active (exists now)
; Consultant:Tricog Health:Active (exists now)
; Consultant:Otsuka:Active (exists now)
; Researcher:Novartis:Active (exists now)
; Consultant:Sumitomo:Active (exists now)
; Consultant:Lexicon:Active (exists now)
; Advisor:Lilly:Active (exists now)
; Advisor:Novo Nordisk:Active (exists now)
; Consultant:Roche Diagnostics:Active (exists now)
; Consultant:Merck:Active (exists now)
; Advisor:Corcept:Active (exists now)
; Consultant:CSL Vifor:Active (exists now)
; Consultant:Boehringer Ingelheim:Active (exists now)
; Consultant:Bayer:Active (exists now)
; Consultant:AstraZeneca:Active (exists now)
| Uchechukwu Ikeaba:DO NOT have relevant financial relationships
| Gregg Fonarow:DO have relevant financial relationships
;
Consultant:AstraZeneca:Active (exists now)
; Consultant:Bayer:Active (exists now)
; Consultant:Novartis:Active (exists now)
; Consultant:Pfizer:Active (exists now)
; Consultant:Merck:Active (exists now)
| Senthil Selvaraj:DO have relevant financial relationships
;
Consultant:BridgeBio:Active (exists now)
; Research Funding (PI or named investigator):Mandel Foundation:Past (completed)
; Research Funding (PI or named investigator):Duke School of Medicine:Active (exists now)
; Research Funding (PI or named investigator):Doris Duke Foundation:Past (completed)
; Research Funding (PI or named investigator):Impetus:Active (exists now)
; Research Funding (PI or named investigator):Foundation for Sarcoidosis Research:Active (exists now)
; Research Funding (PI or named investigator):AHA:Active (exists now)
; Research Funding (PI or named investigator):NHLBI:Active (exists now)
; Consultant:AstraZeneca:Active (exists now)
| Sabra Lewsey:DO NOT have relevant financial relationships
| Ambarish Pandey:DO have relevant financial relationships
;
Consultant:Tricog:Active (exists now)
; Consultant:Sarfez Therapeutics, Edwards Lifesciences, Merck, Bayer, Anumana, Alleviant, Pfizer, Abbott, Axon Therapies, Kilele Health, Acorai, Kardigan, Novartis, Idorsia Pharma, and Science37:Active (exists now)
; Consultant:Rivus:Active (exists now)
; Consultant:iRhythm:Active (exists now)
; Researcher:SQ innovations:Active (exists now)
; Research Funding (PI or named investigator):SC Pharma:Active (exists now)
; Consultant:Astra Zeneca:Active (exists now)
; Research Funding (PI or named investigator):Ultromics:Active (exists now)
; Research Funding (PI or named investigator):Roche:Active (exists now)
; Consultant:Ultromics:Active (exists now)
; Consultant:Roche:Active (exists now)
; Consultant:Lilly:Active (exists now)
; Consultant:Bayer:Active (exists now)
; Consultant:Novo Nordisk:Active (exists now)
| Michel Khouri:No Answer
| Brooke Alhanti:DO NOT have relevant financial relationships
| Jim McDermott:DO have relevant financial relationships
;
Employee:AstraZeneca:Active (exists now)