Outcomes of Heart Failure in Muscular Dystrophies in Adults: A Nationwide Analysis in the United States
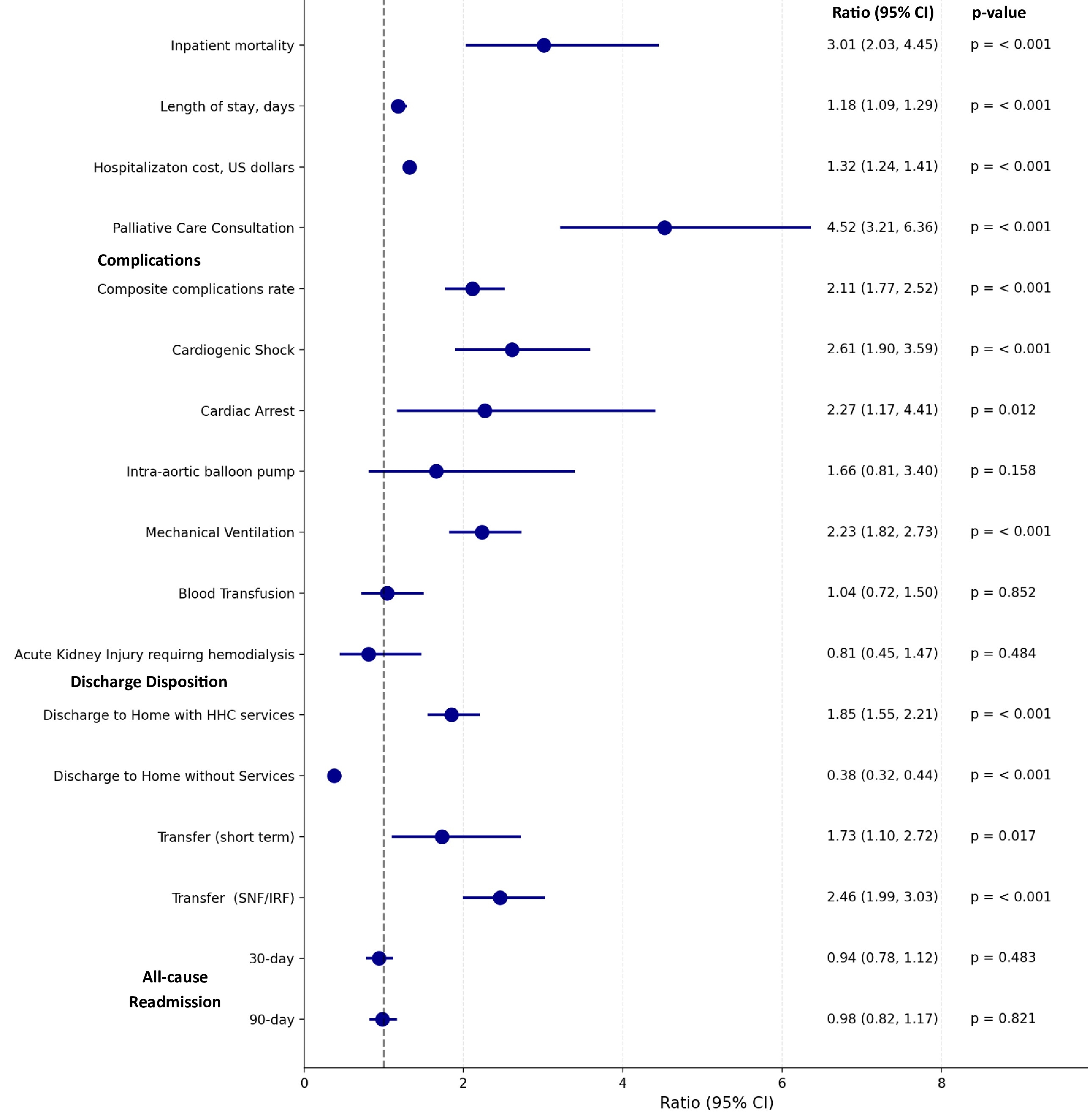
Abstract Body (Do not enter title and authors here): Background: Muscular dystrophies (MDs) may cause heart failure (HF), but outcomes specific to MD-related HF are not well characterized. Research Question: Do the outcomes of HF hospitalizations differ between patients with underlying MDs (MD-HF) vs. patients without MDs (non-MD-HF) in the United States? Methods: Discharge data from HF hospitalizations were abstracted from the Nationwide Readmissions Database (2016-2022) and stratified by the presence or absence of MD (MD-HF vs. non-MD-HF). Logistic regression and lognormal models were estimated to assess differences in inpatient mortality, length of stay (LOS), total costs, complications, and 30-day and 90-day all-cause readmissions. Propensity-score matching (PSM) was used to control baseline differences between the MD-HF and non-MD-HF cohorts. Odds ratios (OR) with associated 95% Confidence intervals (CI) and p-values were reported. Analyses were conducted via SAS v. 9.4, with statistical significance indicated by two-tailed p<.05. Results: 8,466,806 HF hospitalizations were included in the analysis, of which 3688 (0.04%) involved patients with MD. MD-HF hospitalizations involved younger patients (mean age 55.3 vs. 71.3 years, p<0.001) with higher rates of HF with reduced ejection fraction (HFrEF) compared to non-MD-HF hospitalizations (48.1% vs. 34.9%, p<0.001). Compared to non-MD-HF hospitalizations (2.01%), MD-HF hospitalizations (5.82%) were associated with significantly higher odds of inpatient mortality (OR 3.01, 95% CI: 2.03, 4.45); higher complications rate (OR 2.11, 95% CI, 1.77, 2.52) including cardiogenic shock (OR 2.61, 95% CI, 1.90, 3.59), cardiac arrest (OR 2.27, 95% CI, 1.17, 4.41), use of mechanical ventilation (OR 2.23, 95% CI, 1.82, 2.73); higher palliative care consultation (OR 4.52, 95% CI, 3.21, 6.36); as well as more extended hospital LOS (OR 1.18, 95% CI, 1.09, 1.29), higher total costs (OR 1.32, 95% CI, 1.24, 1.41), and higher odds of discharge to rehab facility (OR 2.46, 95% CI, 1.99, 3.03) and home healthcare (OR 1.85, 95% CI, 1.55, 2.21) (all p<0.001). MD was not associated with a significant difference in 30-day (OR 0.94, 95% CI, 0.78, 1.12) and 90-day (OR 0.98, 95% CI, 0.82, 1.17) all-cause readmission rates. Conclusion: MD-HF hospitalizations were associated with higher inpatient mortality, complication rates, resource utilization, discharge to rehab facility and home healthcare, and no difference in readmission rates compared to non-MD-HF hospitalizations.
Abdul Jabbar, Ali Bin
(
Creighton University School of Medicine
, Omaha , Nebraska , United States )
Al-salahat, Ali
(
Creighton University School of Medicine
, Omaha , Nebraska , United States )
Dilsaver, Danielle B.
(
Creighton University School of Medicine
, Omaha , Nebraska , United States )
Ismayl, Mahmoud
(
Mayo Clinic
, Rochester , Minnesota , United States )
Goldsweig, Andrew
(
Baystate Medical Center
, West Hartford , Connecticut , United States )
Aboeata, Ahmed
(
Creighton University School of Medicine
, Omaha , Nebraska , United States )
Author Disclosures:
Ali Bin Abdul Jabbar:DO NOT have relevant financial relationships
| Ali Al-Salahat:No Answer
| Danielle B. Dilsaver:DO NOT have relevant financial relationships
| Mahmoud Ismayl:DO NOT have relevant financial relationships
| Andrew Goldsweig:DO have relevant financial relationships
;
Consultant:Philips:Past (completed)
; Consultant:Occlutech:Active (exists now)
; Consultant:Conformal Medical:Active (exists now)
; Speaker:Boston Scientific:Past (completed)
; Consultant:Abbott:Past (completed)
| Ahmed Aboeata:No Answer