Is Age Just a Number? A Nationwide Multicenter Analysis of Post-Ablation Safety in Elderly Atrial Fibrillation Patients
Abstract Body (Do not enter title and authors here): Background Evidence regarding the safety profile of atrial fibrillation (AF) catheter ablation remains limited. As life expectancy increases, a rising number of elderly patients are considered candidates for this procedure.
Research Question What is the safety profile of AF ablation in elderly patients with new AF in a real-world setting?
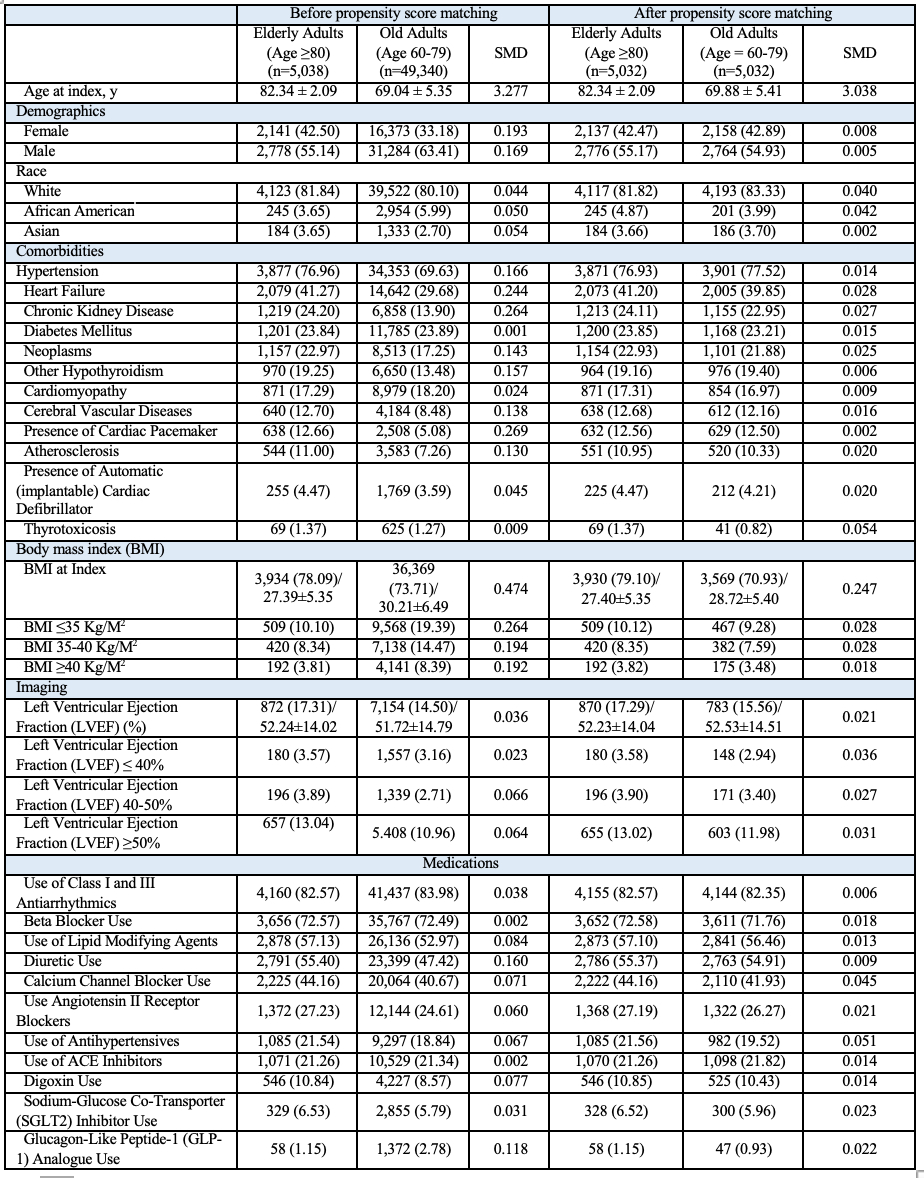
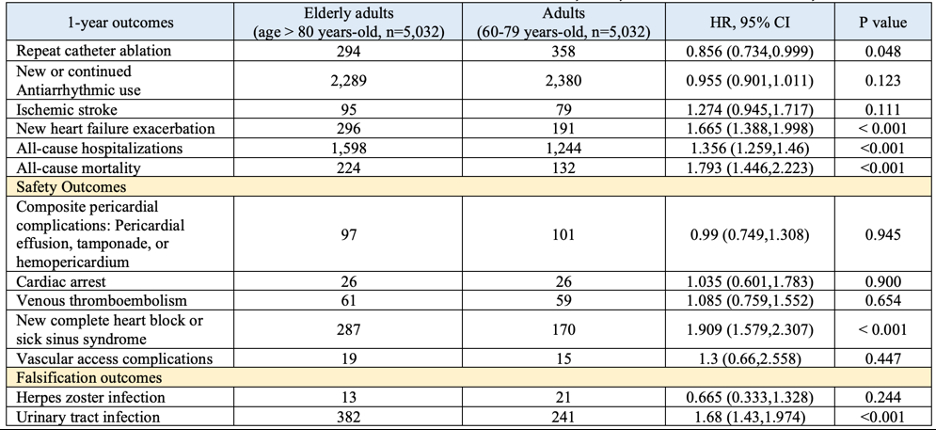
Methods In this U.S.-based multicenter cohort study (TriNetX dataset), we identified adults (≥ 60 years old) with new AF who underwent catheter ablation within 6 months. Patients were grouped by age at first AF episode: 60–79 years (older adults) and ≥80 years (elderly adults). Patients with prior surgical ablation were excluded. Propensity score matching (1:1) balanced groups by demographics, comorbidities, and medications. The primary end point was repeat AF ablation at 1-year; secondary endpoints included new or ongoing antiarrhythmic (AAD) use, ischemic stroke, safety outcomes of heart failure (HF) exacerbations, pericardial complications (pericardial effusion, tamponade or hemopericardium), new venous thromboembolism (VTE), cardiac arrest, conduction disease (new complete heart block or sick sinus syndrome), vascular access complications (post-procedural hematomas or aneurysms), all-cause hospitalizations, and all-cause mortality. Falsification outcomes included urinary tract infections (UTI) and herpes zoster. Kaplan-Meier analysis and log-rank tests compared outcomes; hazard ratios (HRs) with 95% CI were calculated using Cox regression.
Results After matching (N= 5,032 per group), elderly adults were less likely to undergo repeat catheter ablation at 1-year. AAD use and VTE risks were similar between groups. Elderly adults had higher risk of ischemic stroke (HR=1.27, 95% CI = 0.91-1.01, p=0.12) and HF exacerbation (HR=1.67, 95% CI=1.39-2.0, p<0.01). Safety outcomes were similar, however elderly adults were at risk of new conduction disease (HR=1.91, 95% CI = 1.58-2.31, p<0.01). Elderly adults were more likely to be hospitalized (HR= 1.36, 95% CI = 1.26-1.46, p<0.01) and had higher risk of mortality (HR=1.78, 95% CI=1.45-2.22, p<0.01). Falsification outcomes found elderly adults had higher UTI risk (HR=1.68, 95% CI=1.43-1.97, p<0.01).
Conclusion Elderly adults (≥80 years) undergoing catheter ablation had significantly higher risk of complications compared to older adults (60-79 years), underscoring the need for further investigations to mitigate periprocedural risk in AF catheter ablation.
Wang, Yu-chiang
(
University of Hawaii
, Honolulu , Hawaii , United States )
Hsieh, Rebecca
(
Danbury Hospital
, Danbury , Connecticut , United States )
Lee, Pei-lun
(
Jacobi Medical Center
, Bronx , New York , United States )
Chi, Kuan Yu
(
Jacobi Medical Center
, Bronx , New York , United States )
Kumar, Agara
(
Danbury Hospital
, Danbury , Connecticut , United States )
Ahuja, Rahul
(
University of Hawaii
, Honolulu , Hawaii , United States )
Rattanawong, Pattara
(
Massachusetts General Hospital
, Boston , Massachusetts , United States )
Author Disclosures:
Yu-Chiang Wang:DO NOT have relevant financial relationships
| Rebecca Hsieh:DO NOT have relevant financial relationships
| Pei-Lun Lee:DO NOT have relevant financial relationships
| Kuan Yu Chi:DO NOT have relevant financial relationships
| Agara Kumar:No Answer
| Rahul Ahuja:No Answer
| Pattara Rattanawong:No Answer
Khan Muhammad Aslam, Haider Taimoor, Bhattarai Shraddha, Afzal Hafsa, Khan Bilal, Muhammad Anza, Shafique Nouman, Bhatia Hitesh, Aafreen Asna, Adil Abid Nawaz Khan, Akbar Usman, Khan Alamzaib, Haider Muhammad Adnan