Transthoracic Echocardiographic and AI-ECG Predictors of Atrial Arrhythmia Recurrence After Surgical Ablation
Abstract Body (Do not enter title and authors here): Background Atrial arrhythmia recurrence after surgical ablation remains challenging to predict and integrating novel biomarkers may improve risk stratification.
Objective: To evaluate whether combining preoperative transthoracic echocardiography (TTE) with artificial intelligence-enabled ECG (AI-ECG) scores enhances prediction of atrial fibrillation/flutter (AF/AFl) recurrence post surgical ablation.
Methods: We retrospectively analyzed 1,696 patients undergoing Surgical AF/AFl Ablation between 2006 and 2025 with preoperative TTE and post-blanking ECGs. Clinical variables, TTE indices, and AI-ECG scores (AF probability, ECG-estimated age, HFpEF, LV dysfunction, and aortic stenosis scores) were assessed. The primary outcome was time to AF/AFl recurrence. Univariate/multivariable Cox models and a Random Survival Forest (RSF) model (80:20, training: testing) were developed to identify predictors.
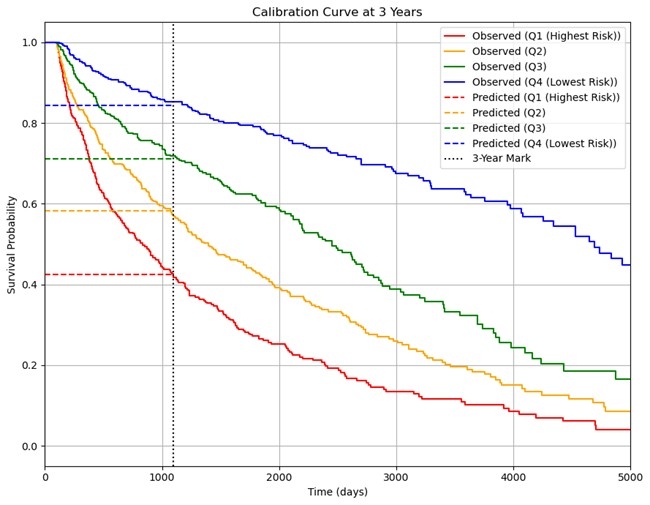
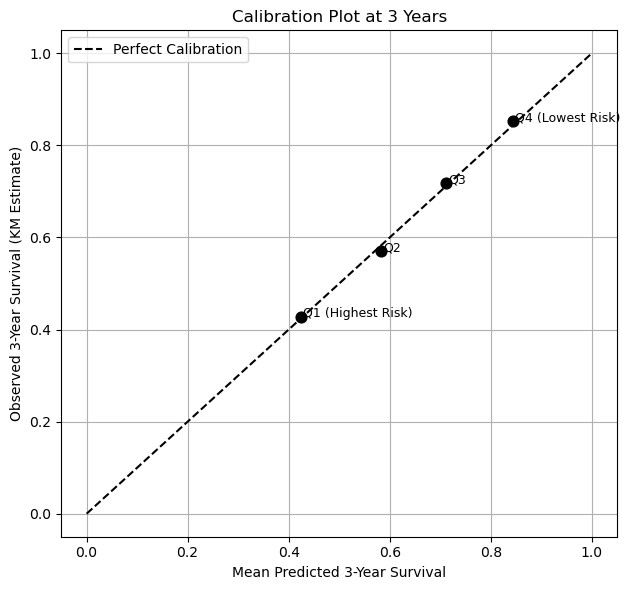
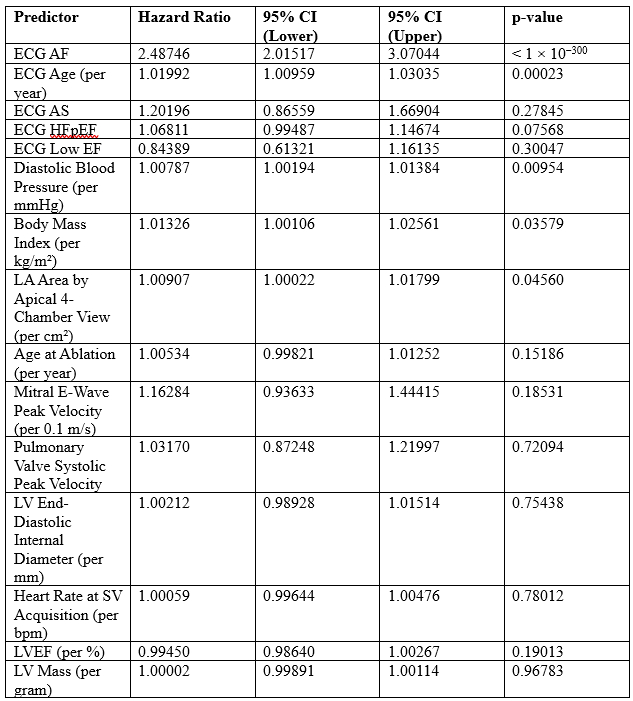
Results: Of 1,696 patients (mean age 67.3±10.2 years; 61.7% male) undergoing surgical AF/AFl ablation, 949 (56%) experienced AF/AFl recurrence during a median follow-up of 3.14 years. Patients with recurrence had larger left atria (mean LA area 30.4 vs 24.5 cm2, p < 0.001), more diastolic dysfunction (mitral inflow E-wave velocity 1.015 m/s vs 0.896 m/s , p < 0.001), and adverse AI-ECG biomarkers. In multivariable analysis, independent predictors of recurrence included a higher ECG-AF score (p < 1 x 10-300), an older AI-ECG age (p = 0.0002), LA area (p = 0.046), body mass index (p = 0.036), and elevated diastolic blood pressure (HR 1.008 per mmHg, 95% CI 1.002 – 1.014; p = 0.010). The final Cox model achieved a C-index of ~0.67 and stratified patients into risk quartiles with 3-year freedom-from-arrhythmia rates of ~85% (lowest-risk) vs ~43% (highest-risk). An RSF model yielded a slightly higher test C-index (≈0.69), suggesting modest improvement with non-linear modeling.
Conclusions: Preoperative AI-ECG biomarkers (AF probability, age discordance) and TTE markers of atrial remodeling independently predicted AF/AFl recurrence after surgical AF/AFl ablation and integration of these metrics improved risk stratification.
Goings, Dylan
(
Mayo Clinic
, Rochester , Minnesota , United States )
Haq, Ikram
(
Mayo Clinic
, Rochester , Minnesota , United States )
Attia, Zachi
(
Mayo Clinic
, Rochester , Minnesota , United States )
Brandt, Michael
(
Mayo Clinic
, Rochester , Minnesota , United States )
Friedman, Paul
(
Mayo Clinic
, Rochester , Minnesota , United States )
Noseworthy, Peter
(
Mayo Clinic
, Rochester , Minnesota , United States )
Killu, Ammar
(
Mayo Clinic
, Rochester , Minnesota , United States )
Author Disclosures:
Dylan Goings:DO NOT have relevant financial relationships
| Ikram Haq:No Answer
| Zachi Attia:No Answer
| Michael Brandt:DO NOT have relevant financial relationships
| Paul Friedman:DO have relevant financial relationships
;
Other (please indicate in the box next to the company name):Anumana:Active (exists now)
; Other (please indicate in the box next to the company name):Eko Health:Active (exists now)
; Other (please indicate in the box next to the company name):AliveCor:Active (exists now)
| Peter Noseworthy:DO have relevant financial relationships
;
Royalties/Patent Beneficiary:Anumana:Active (exists now)
| Ammar Killu:DO NOT have relevant financial relationships