Ablation versus Anti-arrhythmic Drug Therapy for Ventricular Tachycardia in Patients with Ischemic Heart Disease: A Systematic Review and Meta-analysis of Randomized Controlled Trials
Abstract Body (Do not enter title and authors here):
Background. Recurrent ventricular tachycardia (VT) is common in patients with ischemic heart disease (IHD), even with anti-arrhythmic drugs on board. While ICDs can abort VT episodes, ICD shocks can be painful. Ablation therapy can reduce the number of ICD shocks and interventions, but the optimal ablation technique is still uncertain.
Purpose. We aim to review the clinical efficacy and safety of catheter ablation vs anti-arrhythmic drugs in patients with IHD.
Methods. We conducted comprehensive searches across PubMed, CENTRAL, WOS, Scopus, and EMBASE until Feb 2024. Pooled data were reported using risk ratio (RR) for dichotomous outcomes and mean difference (MD) for continuous outcomes, along with a 95% confidence interval (CI). This systematic review and meta-analysis was registered with PROSPERO ID: CRD42024551760.
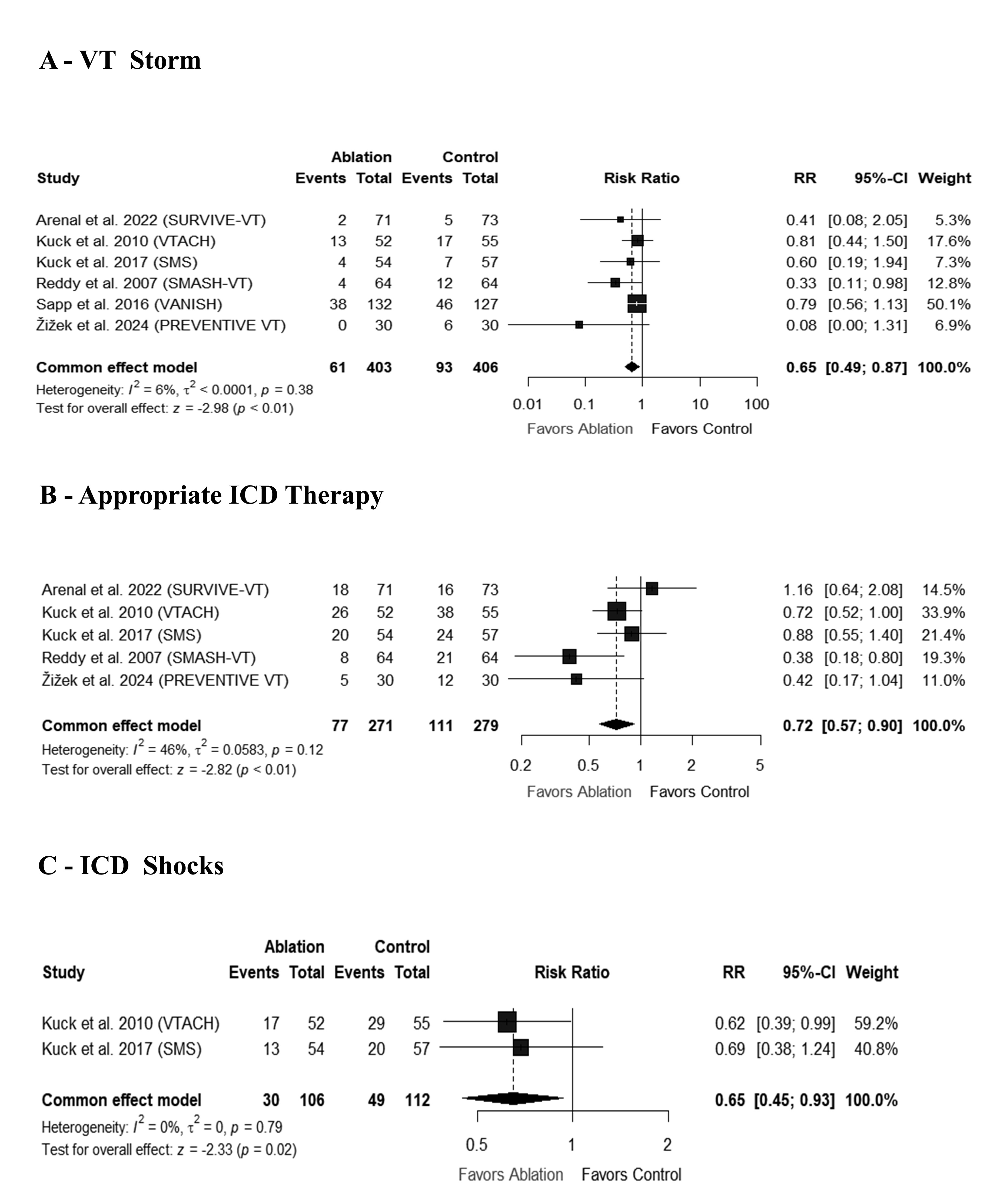
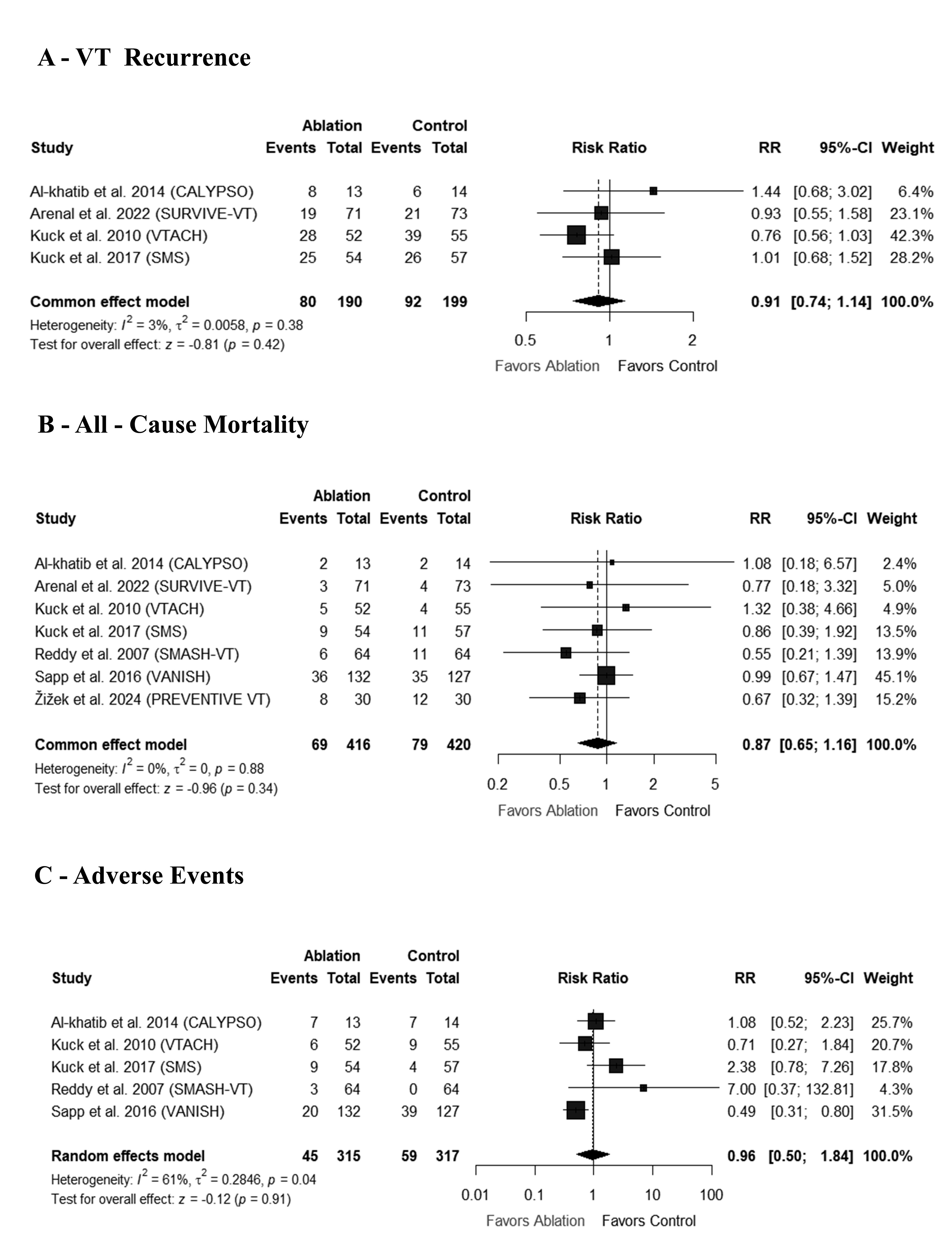
Results. We included seven RCTs with a total of 836 patients. Patients who underwent ablation had a lower risk of VT storm compared to those who received anti-arrhythmic drugs [RR: 0.65 with 95% CI (0.49, 0.87), P < 0.01), Compared to anti-arrhythmic drugs, the catheter ablation group also required less Appropriate ICD therapy [RR: 0.72 with 95% CI (0.57, 0.90), P < 0.01), and fewer ICD shocks [ RR: 0.64 with 95% CI (0.45, 0.93), P = 0.02). However, there was no significant difference in VT recurrence [RR: 0.91 with 95% CI (0.74, 1.14), P = 0.42), all-cause mortality [RR: 0.87 with 95% CI (0.65, 1.16), P = 0.34), or any adverse events [RR: 0.96 with 95% CI (0.50, 1.84), P = 0.91) between the two groups.
Conclusion. Our meta-analysis showed that catheter ablation was associated with a reduction in VT storm, ICD therapy, and ICD shocks. However, when compared to anti-arrhythmic drugs, catheter ablation for VT in IHD patients did not appear to afford any significant survival advantage. ge.
Khan, Ubaid
(
University of Maryland School of Medicine
, Baltimore , Maryland , United States )
Amin, Ahmed Mazen
(
Mansoura University
, Mansoura , Egypt )
A. Ibrahim, Ahmed
(
Faculty of medicine menoufia university
, Cairo , Egypt )
Imran, Muhammad
(
University of Lahore
, Lahore , Pakistan )
Rakab, Mohamed
(
Mansoura University
, Mansoura , Egypt )
M. Albarakat, Majd
(
Jordan University of Science and Technology
, Irbid , Jordan )
Ranabhat, Chet
(
UMMC midtown campus
, Baltimore , Maryland , United States )
Brilliant, Justin
(
University of Maryland School of Medicine
, Baltimore , Maryland , United States )
Chaudhry, Kashif
(
UPMC Williamsport
, Williamsport , Pennsylvania , United States )
Author Disclosures:
Ubaid Khan:DO NOT have relevant financial relationships
| Kashif Chaudhry:No Answer
| Ahmed Mazen Amin:DO NOT have relevant financial relationships
| Ahmed A. Ibrahim:DO NOT have relevant financial relationships
| Muhammad Imran:DO NOT have relevant financial relationships
| Mohamed Rakab:DO NOT have relevant financial relationships
| Arej Iltaf:DO NOT have relevant financial relationships
| Majd M. AlBarakat:DO NOT have relevant financial relationships
| Chet Ranabhat:DO NOT have relevant financial relationships
| Justin Brilliant:DO NOT have relevant financial relationships