When Drainage Backfires: Pericardial Decompression Syndrome in an ESRD Patient
Abstract Body (Do not enter title and authors here): Introduction
End stage renal disease (ESRD) patients may develop pericardial effusion due to fluid overload from inadequate dialysis. Large effusions, when drained, can cause pericardial decompression syndrome, a rare complication involving paradoxical hemodynamic collapse. This case highlights the challenges with management of a large pericardial effusion in an ESRD patient.
Case Description
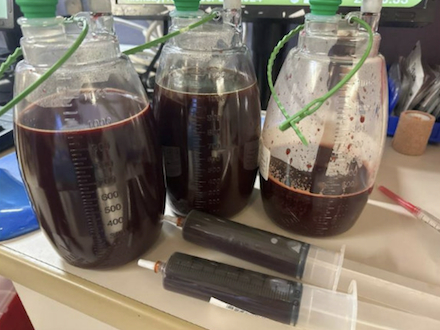
A 44 year old male with ESRD on intermittent hemodialysis (iHD) presented with chest pain and systolic blood pressure in the 80s. Exam showed jugular venous distension. Transthoracic echocardiogram revealed a large pericardial effusion without tamponade (Figure A). Pericardiocentesis drained 2.5 liters of sanguineous fluid (Figure B). Post procedure, the patient's mean arterial pressure decreased beneath 65 mmHg. Bedside echocardiogram was concerning for right ventricular dilation. The drain was temporarily clamped, and the patient received vasopressors. He underwent continuous renal replacement therapy (CRRT) for fluid optimization before returning to iHD with improved ultrafiltration goals. By day seven, the drain produced less than 50 mL of fluid over the previous twenty-four hours. Bedside echocardiogram was confirmatory, so the drain was removed. The patient was discharged with outpatient cardiology follow-up.
Discussion
Despite the large effusion, the absence of tamponade suggests chronic fluid accumulation, allowing gradual pericardial stretch, reduced intra-pericardial pressure change, and hemodynamic compensation. In this patient, pericardial decompression syndrome occurred from suddenly increased venous return, rapid right sided expansion (as shown on bedside echocardiogram), septal shift, left ventricular compression, decreased output, and ultimately hypotension. Another factor may have been the sudden change in preload with relatively unchanged systemic vascular resistance, thus preload/afterload mismatch. The effusion was likely due to insufficient fluid removal during dialysis, emphasizing the importance of dialysis quality in preventing cardiac complications. However, decompression syndrome is rare, with less than 5% incidence among patients who undergo drainage.
Conclusion
Inadequate dialysis predisposes to fluid overload, which can cause large pericardial effusion. While tamponade may be absent, large effusions propose the risk of decompression syndrome with drainage. Optimal dialysis and close hemodynamic monitoring were critical in this patient's recovery.
Abdel Aziz, Khaled
(
University of Cincinnati
, Cincinnati , Ohio , United States )
Kotei, Charlene
(
University of Cincinnati
, Cincinnati , Ohio , United States )
Tejan Sie, Ahmad
(
University of Cincinnati
, Cincinnati , Ohio , United States )
Sultan, Hamza
(
University of Cincinnati
, Cincinnati , Ohio , United States )
Slifer, Damian
(
Allegheny Health Network
, Pittsburgh , Pennsylvania , United States )
Khokhlov, Leonid
(
University of Cincinnati
, Cincinnati , Ohio , United States )
Khan, Naseer
(
University of Cincinnati
, Cincinnati , Ohio , United States )
Author Disclosures:
Khaled Abdel Aziz:DO NOT have relevant financial relationships
| Charlene Kotei:No Answer
| Ahmad Tejan Sie:No Answer
| Hamza Sultan:DO NOT have relevant financial relationships
| Damian Slifer:DO NOT have relevant financial relationships
| Leonid Khokhlov:DO NOT have relevant financial relationships
| Naseer Khan:DO NOT have relevant financial relationships