A Case of Possible IgG4-Related Constrictive Pericarditis Masquerading as Idiopathic Pericarditis: A Rare and Elusive Diagnosis
Abstract Body (Do not enter title and authors here):
Background: Constrictive pericarditis (CP) impairs diastolic filling, commonly manifesting as right-sided heart failure. Immunoglobulin G4-related disease (IgG4-RD) is an immune-mediated fibroinflammatory condition that can affect virtually every organ system and rarely cause CP.
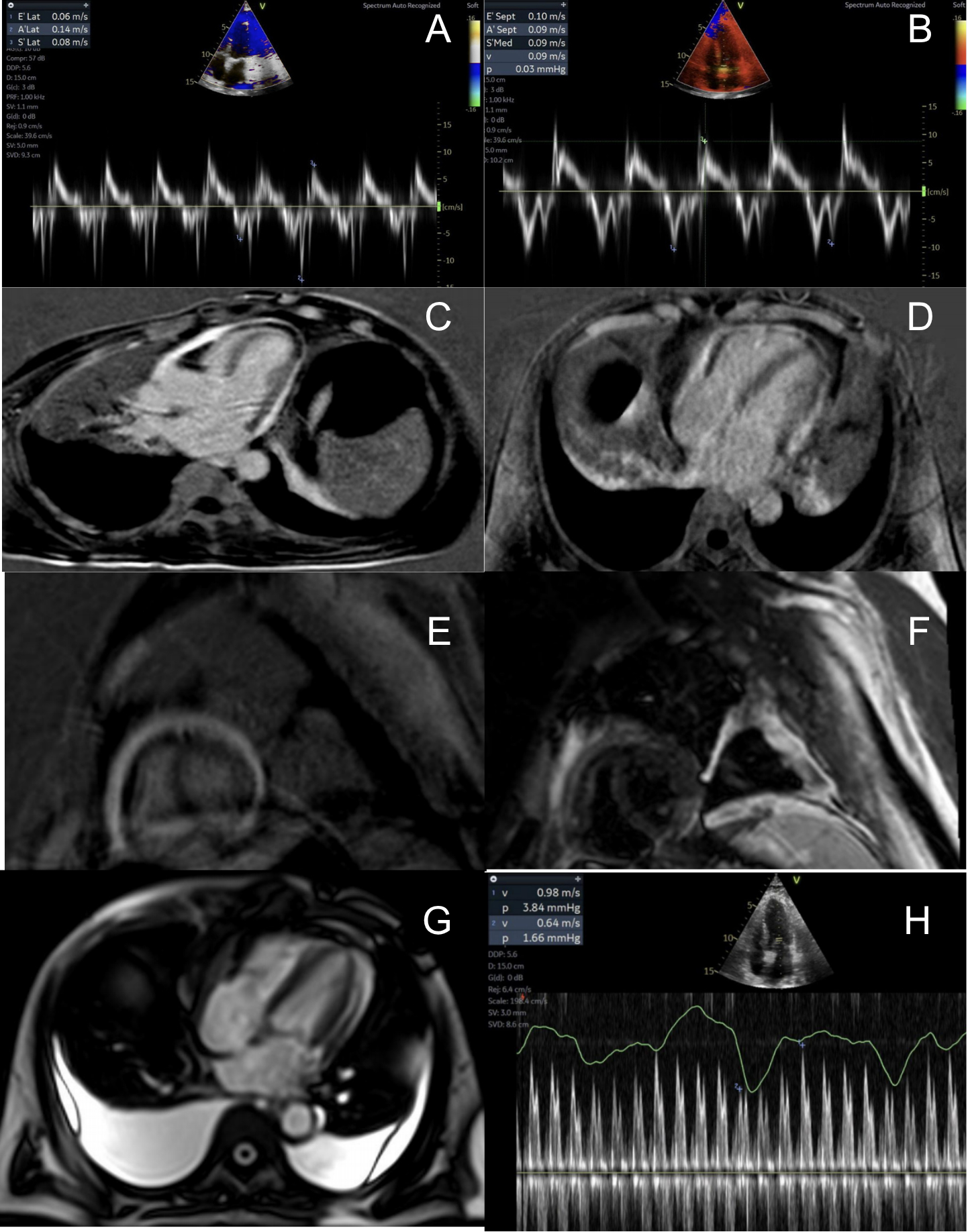
Case Presentation: A 62-year-old man from India presented with insidious onset dyspnea, leg swelling, abdominal distension and weight gain. Physical exam revealed pedal edema, tense ascites, and Kussmaul’s sign. Initial labs showed cholestatic liver injury pattern. Imaging demonstrated bilateral pleural effusions, pericardial effusion, liver cirrhosis, and splenomegaly. Pleural fluid showed exudate, and high SAAG, low protein ascites were noted. Transthoracic echocardiogram (TTE) with Doppler showed septal bounce, annulus reversus, increased respiratory variation in mitral inflow E velocity, and atrial systolic notch on M-mode of the interventricular septum. Cardiac Magnetic Resonance imaging demonstrated patchy T2 hyperintensity with diffuse late gadolinium enhancement out of proportion to T2. Right heart catheterization (RHC) confirmed elevated and equalized diastolic pressures, confirming the diagnosis of CP. Despite the high initial concern for TB, extensive microbiological workup was negative. Absence of cavitary lung lesions, neutrophil-predominant pleural effusion, and an uncharacteristic ascitic fluid analysis for TB suggested an alternate diagnosis. Liver biopsy showed interface hepatitis, bile duct injury, and bridging fibrosis, suggesting autoimmune hepatitis/cholangitis. Serum IgG4 subclass levels returned markedly elevated at 366.4 mg/dL. Per 2020 Revised Comprehensive Diagnostic Criteria, the patient met clinical and serologic criteria for IgG4-RD. After multidisciplinary discussion regarding risks/benefits, pericardial stripping was not pursued. The patient received diuresis and paracentesis for symptom relief, and ibuprofen with colchicine for pericarditis.
Conclusion: IgG4-RD should remain an important diagnostic consideration in idiopathic CP, especially in the setting of multi-system involvement. In our patient, IgG4-related CP possibly co-occurred with autoimmune cholangitis. While pericardial surgery would yield maximum therapeutic benefit and histopathologic confirmation of the underlying diagnosis, our case highlights a rare form of CP caused by an infiltrative disease process.
Nandyal, Shreyas
(
Cook County Health
, Chicago , Illinois , United States )
Sharma, Bharosa
(
Cook County Health
, Chicago , Illinois , United States )
Gajjar, Rohan
(
Cook County Health
, Chicago , Illinois , United States )
Varma, Revati
(
Cook County Health
, Chicago , Illinois , United States )
Ezegwu, Olisa
(
Cook County Health
, Chicago , Illinois , United States )
Amdetison, Gedion Yilma
(
Cook County Health
, Chicago , Illinois , United States )
Tottleben, Jon
(
Cook County Health
, Chicago , Illinois , United States )
Author Disclosures:
Shreyas Nandyal:DO NOT have relevant financial relationships
| Bharosa Sharma:No Answer
| Rohan Gajjar:No Answer
| Revati Varma:No Answer
| Olisa Ezegwu:No Answer
| Gedion Yilma Amdetison:DO NOT have relevant financial relationships
| Jon Tottleben:DO NOT have relevant financial relationships