Coronary Artery Calcium and Risk of Cardiovascular Events in Immune-Mediated Inflammatory Disease from the CLARIFY No/Low-Cost CT Calcium Score Registry
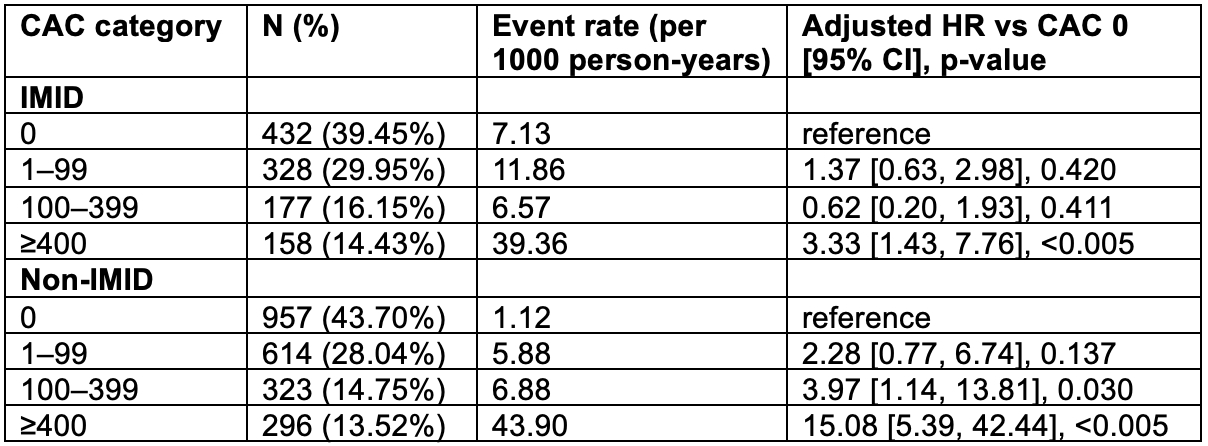
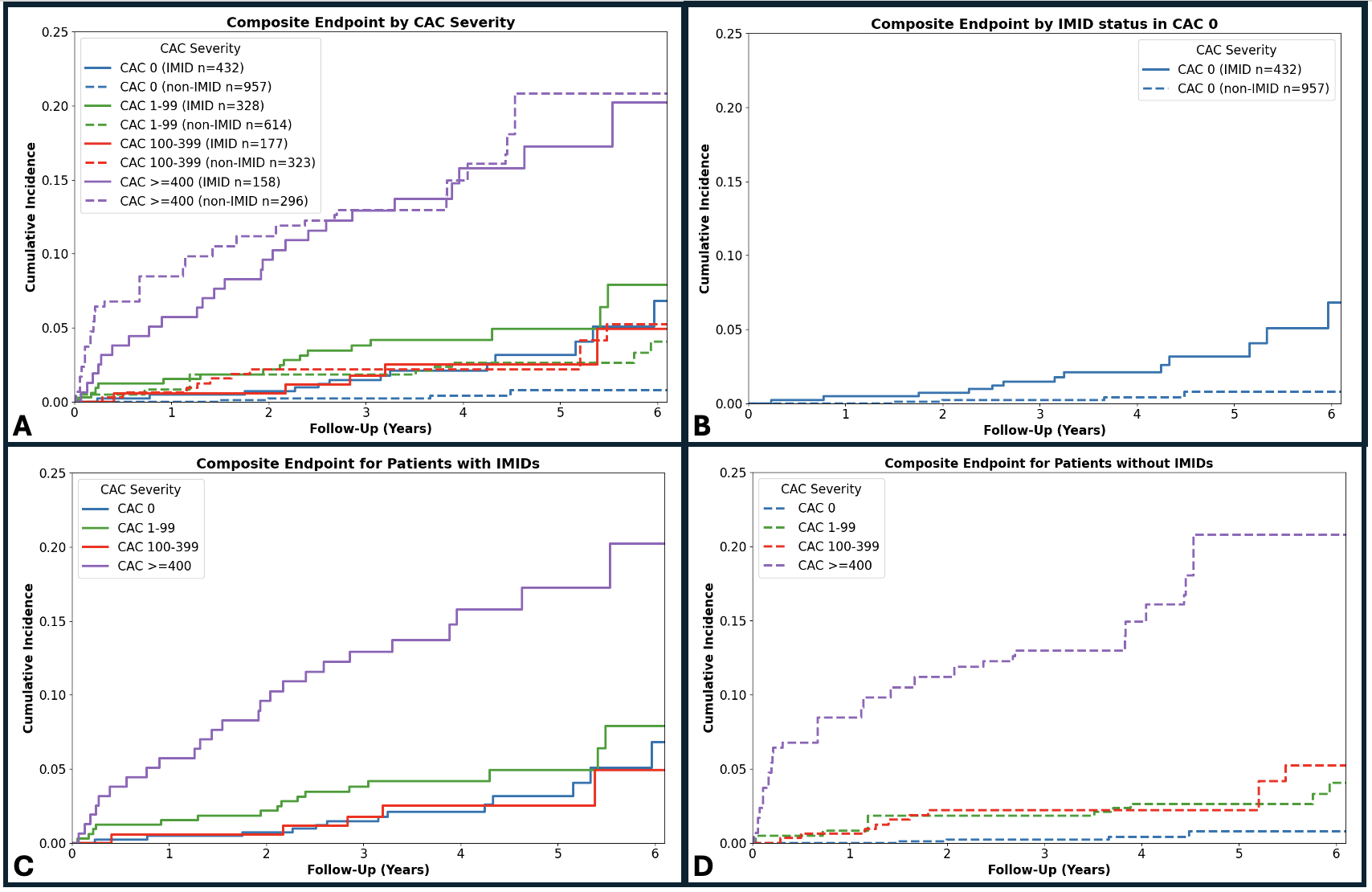
Abstract Body (Do not enter title and authors here): Background. Immune-mediated inflammatory diseases (IMID) accelerate atherosclerosis, yet it is unclear whether coronary artery calcium (CAC) scoring captures this excess cardiovascular risk. Hypothesis. In adults undergoing CT calcium scoring (CTCS), IMID modifies the relationship between CAC score and incident myocardial infarction (MI) or coronary revascularization. Methods. Among 43,420 patients in the CLARIFY Registry (University Hospitals Cleveland, 2014-2020) who underwent no/low-cost CTCS scans, we identified 1095 IMID patients (systemic lupus erythematosus 162, rheumatoid arthritis 557, psoriasis 430) using International Classification of Disease (ICD9/10 codes). After 2:1 propensity matching on age, sex, race, hypertension, diabetes, and smoking status, 3285 matched patients were analyzed (1097 IMID, 2190 controls). CAC was categorized 0, 1–99, 100–399, ≥400, and the primary outcome of incident MI or revascularization was analyzed over a median 4.2-year follow-up. Cox models tested CAC categories compared to CAC 0 stratified by IMID. Additionally, a log(CAC+1) × IMID interaction term was modeled to assess whether the risk gradient of CAC differed by IMID status. Results. Among patients with no coronary calcium, IMID patients experienced a six-fold higher event rate than controls (7.13 vs 1.12 per 1000 person-years). The cumulative incidence curves for IMID patients with zero CAC did not differ significantly from non-IMID patients with CAC 1-99 (log-rank p=0.57) or 100-399 (p=0.84). Within IMID, increases from CAC 0 to CAC 100-399 did not increase the risk (p=0.411), whereas in controls it quadrupled risk (HR=3.97, p=0.005). At CAC ≥400, the cumulative MI/revascularization incidence was similarly high in IMID and controls (log-rank p=0.60). The interaction term was negative (β = –0.93; HR 0.39 [0.27, 0.57]), implying that each log-unit CAC rise multiplies hazard 4-fold in controls but only 1.5-fold in IMID, suggesting a flattened CAC-risk gradient in IMID. Conclusion. In IMID patients, baseline risk is elevated even with zero CAC, with significant attenuation of the traditional CAC-risk gradient observed in controls. These findings suggest that CAC may underestimate cardiovascular risk in IMID patients, who may benefit from more aggressive preventative strategies even when CAC is absent or low.
Singh, Prerna
(
Case Western Reserve University
, Cleveland , Ohio , United States )
Kotanidis, Christos P.
(
BRIGHAM AND WOMENS HOSPITAL
, Boston , Massachusetts , United States )
Shafiabadi Hassani, Neda
(
UNIV HOSP CLEVELAND MEDICAL CTR
, Cleveland , Ohio , United States )
Weber, Brittany
(
BRIGHAM AND WOMENS HOSPITAL
, Boston , Massachusetts , United States )
Wilson, David
(
Case Western Reserve University
, Cleveland , Ohio , United States )
Rajagopalan, Sanjay
(
UNIV HOSP CLEVELAND MEDICAL CTR
, Cleveland , Ohio , United States )
Author Disclosures:
Prerna Singh:DO NOT have relevant financial relationships
| Christos P. Kotanidis:No Answer
| Neda Shafiabadi Hassani:No Answer
| Brittany Weber:DO have relevant financial relationships
;
Advisor:Novo Nordisk :Active (exists now)
; Advisor:BMS :Active (exists now)
; Consultant:Oruka :Past (completed)
; Advisor:Kiniksa :Past (completed)
| David Wilson:DO have relevant financial relationships
;
Ownership Interest:PulseImaging.AI:Active (exists now)
| Sanjay Rajagopalan:DO NOT have relevant financial relationships