Association of Hospital Shock Center Level with In-Hospital Outcomes in Cardiogenic Shock: An Analysis of the Nationwide Readmissions Database
Abstract Body (Do not enter title and authors here): Background: Patients with cardiogenic shock (CS) have high in-hospital mortality. Regionalized systems of care, modeled after trauma and ST-segment-elevation myocardial infarction networks, have been proposed to improve outcomes. Expert consensus frameworks classify CS centers based on mechanical circulatory support (MCS) capabilities, but national outcome data remain limited. This study assessed the association between hospital shock center designation and clinical outcomes.
Methods: Adults (≥18 y) hospitalized with a primary or secondary diagnosis of CS were identified from the Nationwide Readmissions Database (2016–2022). Hospitals were stratified annually into four CS center levels using procedural codes: Level 1 (≥1 durable left ventricular assist device or cardiac transplantation [LVAD/HTx] transplant case), Level 1A (extracorporeal membrane oxygenation, Impella 5.5 or TandemHeart capable without durable LVAD/HTx), Level 2 (percutaneous coronary intervention [PCI]-capable hospitals offering intra-aortic balloon pump [IABP] or Impella CP/RP), and Level 3 (non-PCI, non-MCS hospitals with ICU-level care only). Outcomes included in-hospital mortality, 30-day readmissions, MCS use, length of stay (LOS), and cost. Multinomial overlap propensity and hierarchical regression models were used to adjust and analyze outcomes.
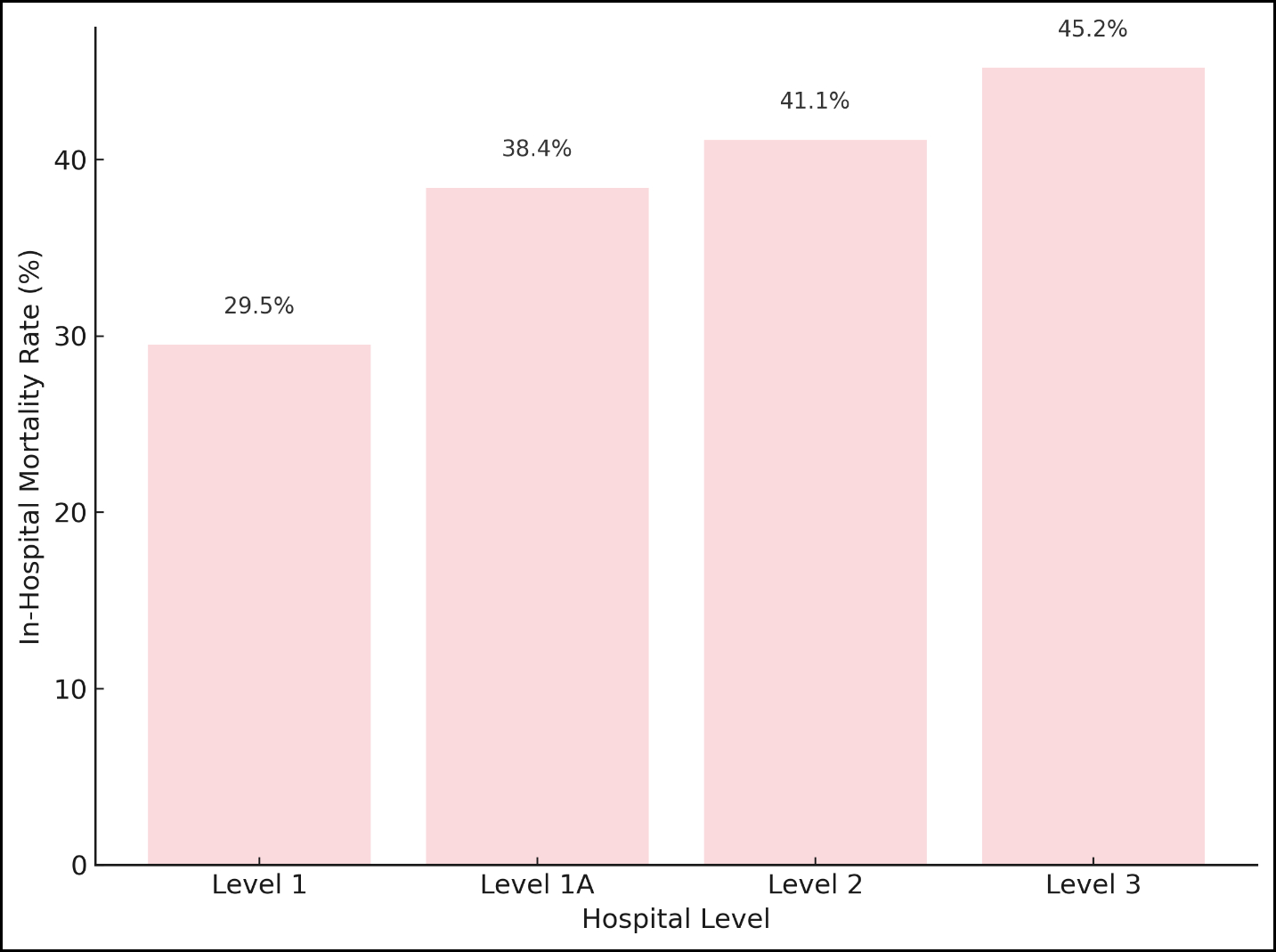
Results: Among 623,835 CS hospitalizations, 33.8% occurred at Level 1, 49.5% at Level 1A, 11.8% at Level 2, and 4.8% at Level 3 centers. After propensity weighting, baseline characteristics were well balanced across shock center levels. In-hospital mortality increased across levels: unadjusted 29.5% at Level 1, 38.4% at Level 1A, 41.1% at Level 2, and 45.2% at Level 3; adjusted analyses vs. Level 1: odds ratio 1.33 [95% CI, 1.29–1.38] for Level 1A; 1.44 [95% CI, 1.38–1.50] for Level 2; 1.63 [95% CI, 1.54–1.71] for Level 3; all p<0.001 (Figure 1). MCS use was highest at Level 1 centers (26.1%) and lowest at Level 2 centers (10.4%). Thirty-day readmission rates were lower at lower-level centers compared to Level 1. LOS and costs were highest at Level 1 centers. Pre-specified subgroup analyses showed consistent survival benefit favoring higher-level centers.
Conclusion: In a large national study, higher tiers of CS centers were associated with improved short-term outcomes independent of patient comorbidity and acuity supporting the need for regionalization of CS care.
Pawar, Shubhadarshini
(
Cedars Sinai Medical Center
, Los Angeles , California , United States )
Bansal, Kannu
(
Saint Vincent Hospital
, Worcester , Massachusetts , United States )
Abbott, J Dawn
(
Warren Alpert Medical School of Brown University
, Providence , Rhode Island , United States )
Katz, Jason
(
New York University Grossman School of Medicine
, New York , New York , United States )
Dudzinski, David
(
Massachuesetts General Hospital/Harvard Medical School
, Boston , Massachusetts , United States )
Van Diepen, Sean
(
University of Alberta
, Edmonton , Alberta , Canada )
Solomon, Michael
(
National Institutes of Health
, Bethesda , Maryland , United States )
Ton, Van-khue
(
Massachuesetts General Hospital/Harvard Medical School
, Boston , Massachusetts , United States )
Vallabhajosyula, Saraschandra
(
Warren Alpert Medical School of Brown University
, Providence , Rhode Island , United States )
Author Disclosures:
Shubhadarshini Pawar:DO NOT have relevant financial relationships
| Kannu Bansal:DO NOT have relevant financial relationships
| J Dawn Abbott:No Answer
| Jason Katz:DO have relevant financial relationships
;
Speaker:Zoll:Past (completed)
; Speaker:Abiomed:Past (completed)
| David Dudzinski:No Answer
| Sean Van Diepen:DO NOT have relevant financial relationships
| Michael Solomon:DO NOT have relevant financial relationships
| Van-Khue Ton:No Answer
| Saraschandra Vallabhajosyula:DO NOT have relevant financial relationships