Utilization of Advanced Diagnostics in Younger Adults with First Unexplained Ventricular Tachycardia, Ventricular Fibrillation or Cardiac: A U.S. Based Multicenter Cohort Study
Abstract Body (Do not enter title and authors here): Background Current studies evaluating diagnostic testing in younger adults with first ventricular fibrillation (VF), tachycardia (VT) or cardiac arrest is largely limited to tertiary centers or designated registries, with few reflecting community practices. Variation in the diagnostic workup for younger adults with first ventricular tachyarrhythmias may lead to under-recognition of treatable or preventable underlying conditions.
Research Question In the real-world setting, how are advanced diagnostics utilized in adult patients under 60 years-old with first VF, VT, or cardiac arrest, and what are the diagnostic yields?
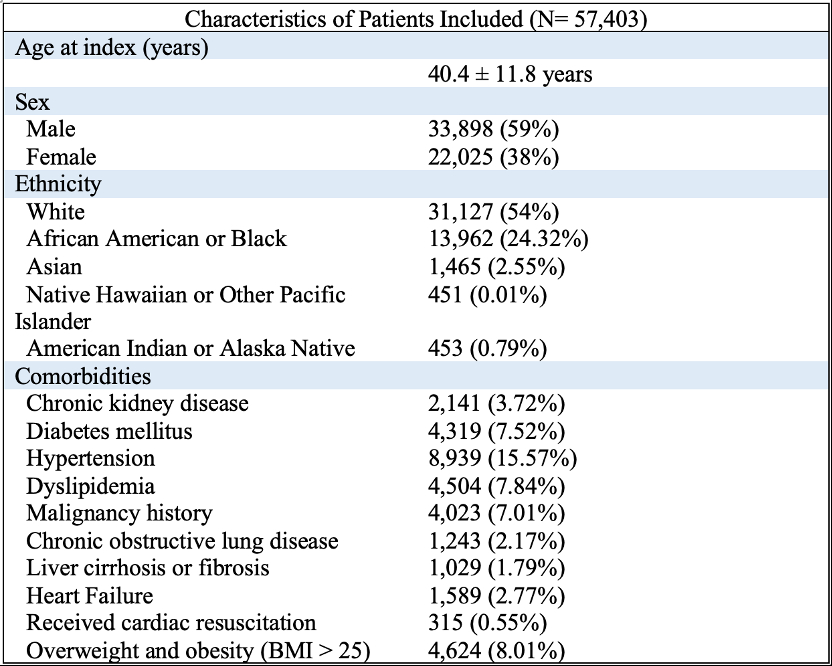
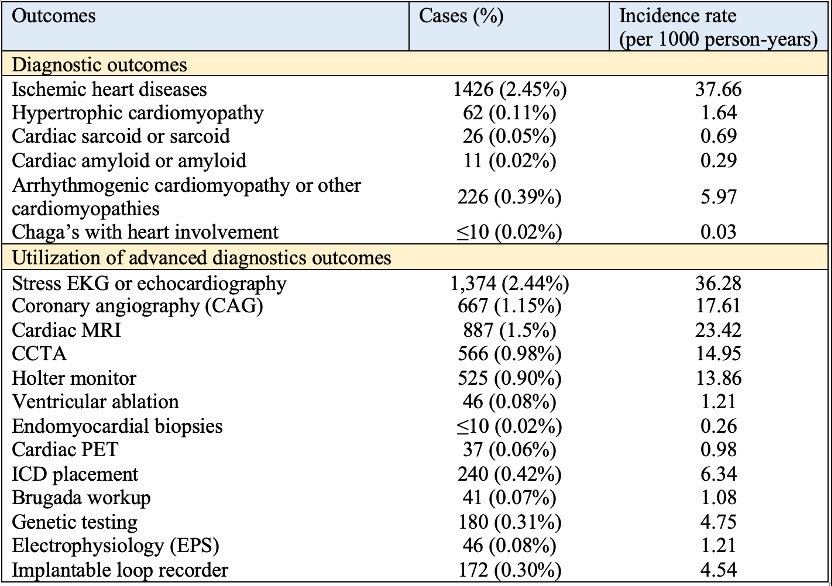
Methods Using a U.S.-based multicenter retrospective database (TriNetX), adults (18 - 60 years), with first VF, VT or cardiac arrest (2019 to 2024) were included (Table 1). Patients with prior implantable cardioverter-defibrillator or pacemakers, ischemic cardiomyopathy, amyloidosis, sarcoidosis, or hypertrophic cardiomyopathy (HCM) were excluded. Outcomes were utilization rates for coronary angiography (CAG), CCTA, cardiac MRI, cardiac PET, myocardial biopsy, genetic testing, exercise ECGs, electrophysiological testing, implantable loop recorder, and diagnostic yield of cardiomyopathies (e.g. sarcoidosis, amyloidosis, HCM, or other channelopathies). Incidence rates were calculated using mean person-time over a 5-year period.
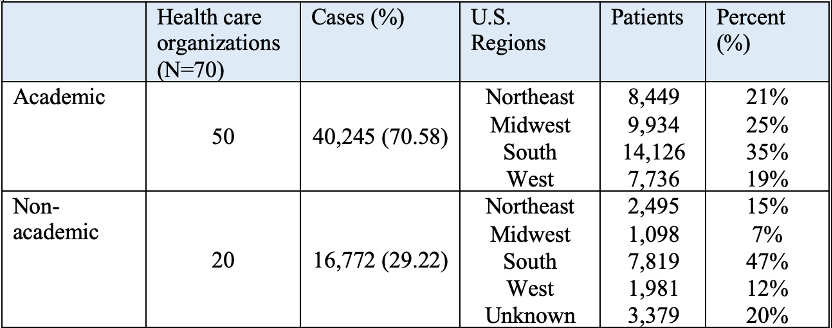
Results A total of 57,403 patients were included, 40,245 (71%) received care at academic institutions. Mean follow-up was 237.70 ± 436.36 days, median follow-up 9 days (IQR: 276 days), totaling 37,310 person-years. The mean age of was 40.4 ± 11.8 years. In these patients, 1,374 (2.44%) received stress EKG or echocardiogram, 887 patients (1.5%) cardiac MRI, 556 (0.98%) CCTA, 180 (0.31%) genetic testing, and 172 (0.30%) received implantable loop recorder evaluation. For diagnostic outcomes, only 1,426 (2.45%) were diagnosed with ischemic heart disease, 226 (0.39%) arrhythmogenic cardiomyopathy or other cardiomyopathies, 62 (0.11%) HCM, 26 (0.05%) with sarcoidosis (Table 2). Incidence rates are presented in Table 2; regional distribution as presented in Table 3.
Conclusions In a large national cohort, advanced diagnostic workups were infrequently performed in younger adults with first ventricular tachyarrhythmias. The brief median follow-up time suggests poor continuity in the real-world setting. This underscores the need for standardized and systemic evaluation pathways to improve outcomes and treat preventable conditions.
Hsieh, Rebecca
(
Danbury Hospital
, Danbury , Connecticut , United States )
Chi, Kuan Yu
(
Jacobi Medical Center
, Bronx , New York , United States )
Lee, Pei-lun
(
Jacobi Medical Center
, Bronx , New York , United States )
Kumar, Agara
(
Danbury Hospital
, Danbury , Connecticut , United States )
Tran, Viet Nghi
(
Weiss Memorial Hospital, Chicago
, Chicago , Illinois , United States )
Wang, Yu-chiang
(
University of Hawaii
, Honolulu , Hawaii , United States )
Author Disclosures:
Rebecca Hsieh:DO NOT have relevant financial relationships
| Kuan Yu Chi:DO NOT have relevant financial relationships
| Pei-Lun Lee:DO NOT have relevant financial relationships
| Agara Kumar:No Answer
| Viet Nghi Tran:DO NOT have relevant financial relationships
| Yu-Chiang Wang:No Answer