Glucagon-Like Peptide-1 Receptor Agonists with Guideline Therapy Lower Mortality and Hospitalizations in HFpEF: A Propensity-Matched U.S. TriNetX Study
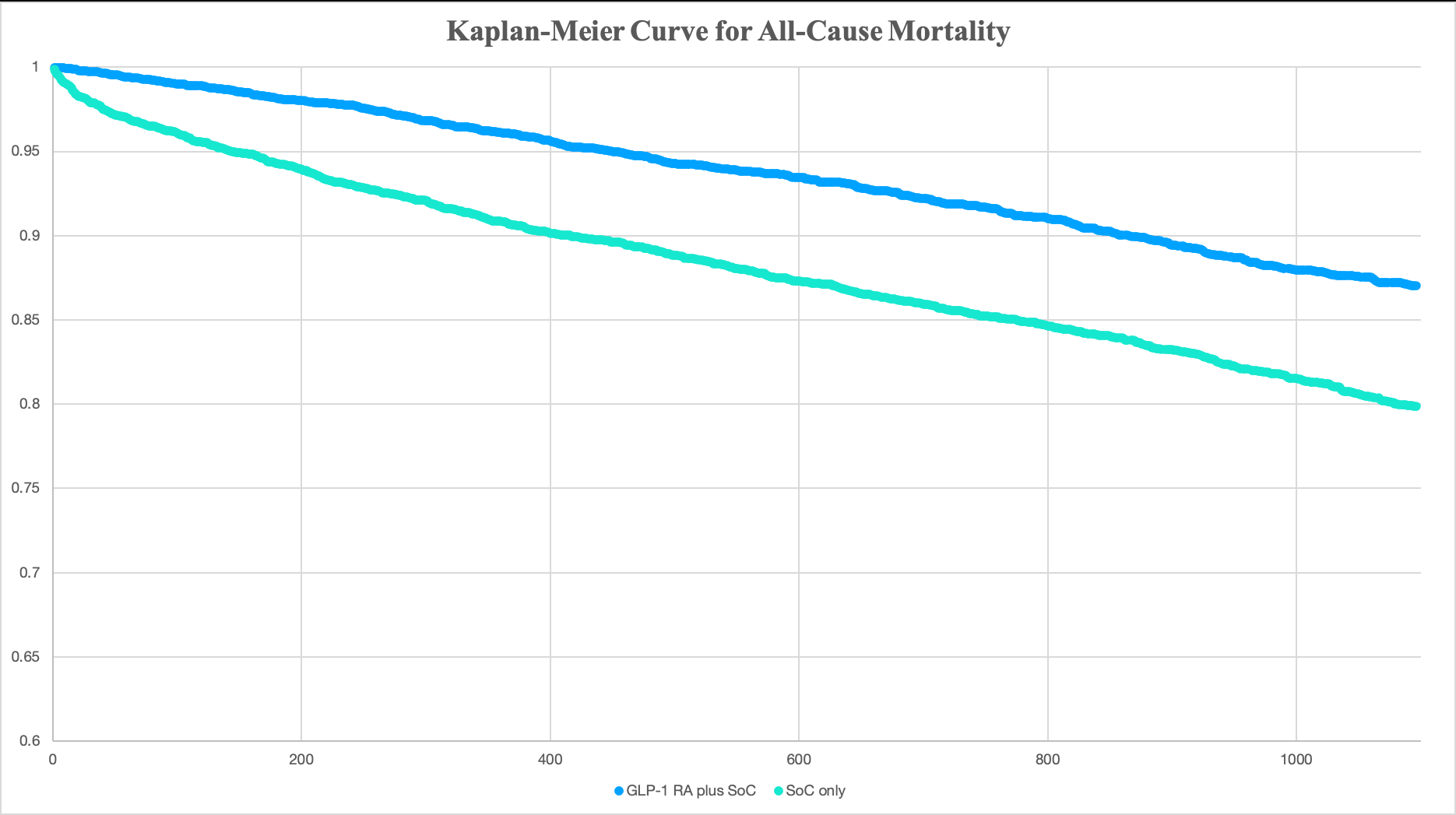
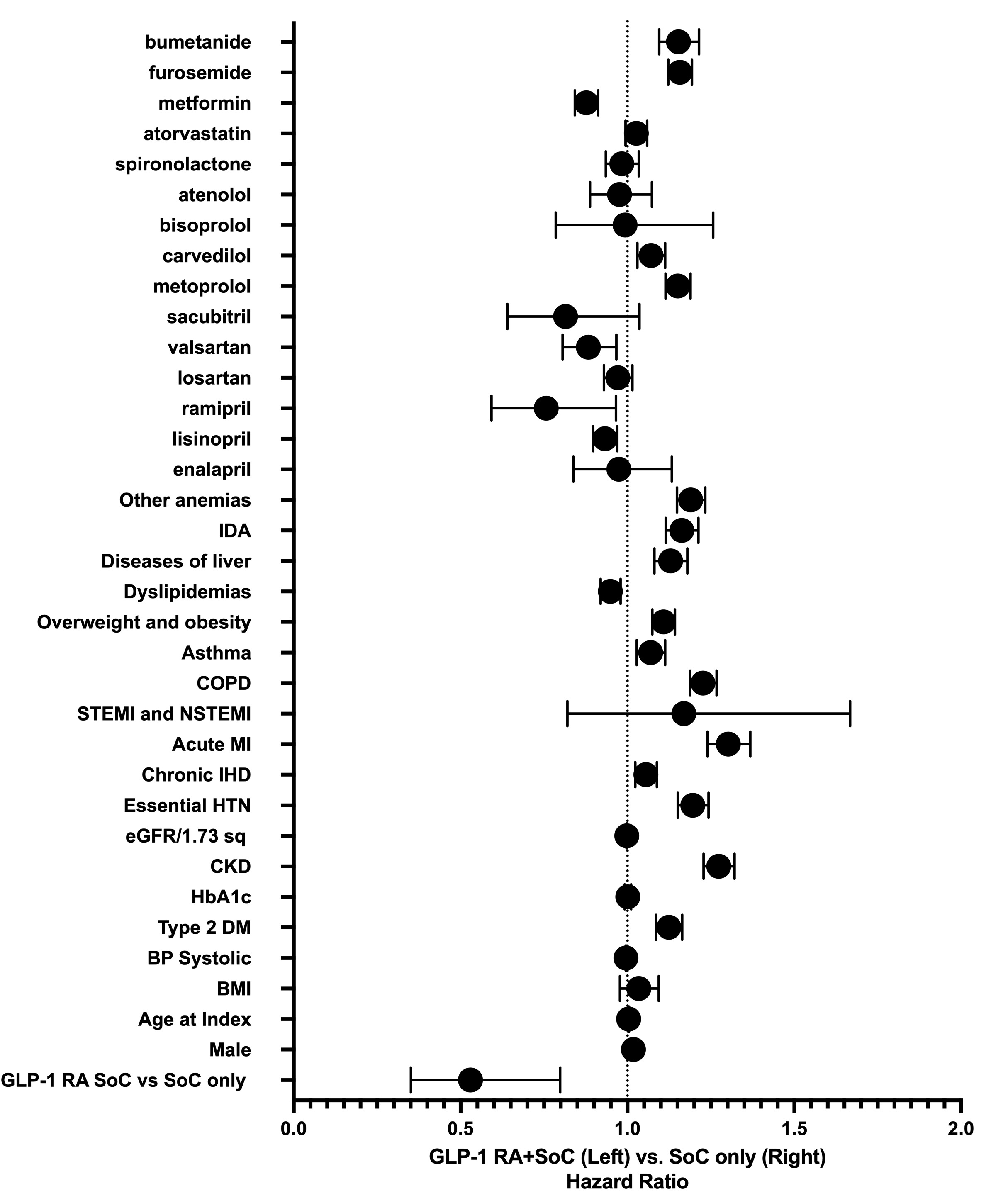
Abstract Body (Do not enter title and authors here): Background Heart failure with preserved ejection fraction (HFpEF) in patients with type 2 diabetes and obesity is common and associated with high morbidity. Glucagon like peptide 1 receptor agonists (GLP-1 RAs) improve weight and glycemic control, but their impact on clinical outcomes in HFpEF remains uncertain. Research Question Does adding GLP1 RAs to standard of care (SoC) pharmacotherapy reduce 3-year all-cause death and hospitalization compared with SoC alone in adults with HFpEF? Methods A retrospective cohort study was conducted using the TriNetX U.S. Collaborative Network (69 HCOs). Adults ≥18 years with HFpEF (LVEF ≥50%), type 2 diabetes, and BMI ≥30 kg/m2 initiating a GLP1 RA between January 2016 and January 2025 were identified. The comparison cohort received SoC therapies without GLP-1 RAs. A one-year look-back period captured baseline comorbidities; outcomes were evaluated for 3 years post-index. One-to-one propensity score matching balanced demographics and 24 comorbidities. Cox proportional-hazards models estimated hazard ratios (HRs) with 95% confidence intervals (CIs). Results After 1:1 propensity matching (N = 5,474/group; mean age 70 ± 11 y; 57% women), GLP1 RA therapy produced fewer all cause deaths than SoC alone (8.9% vs 14.7%; HR 0.56, 95 % CI 0.51–0.63, p < 0.001) and fewer hospitalizations (49.1% vs 66.2%; HR 0.54, 95% CI 0.51–0.56, p < 0.001). GLP-1 RAs also lowered the risk of AKI (HR 0.70, 95% CI 0.63–0.79, p < 0.001), atrial fibrillation/flutter (HR 0.59, 95% CI 0.51–0.69, p < 0.001), AMI (HR 0.63, 95% CI 0.54–0.73, p < 0.001), and progression to dialysis (HR 0.61, 95% CI 0.54–0.68, p < 0.001). ER visits fell modestly (HR 0.85, 95 % CI 0.81–0.89, p = 0.001), whereas ED encounters increased (HR 2.00, 95 % CI 1.82–2.21, p < 0.001). Median follow-up was 2.3 y (IQR 1.9–3.0), and proportional-hazards assumptions held. Conclusions Among U.S. adults with HFpEF, diabetes, and obesity, adding a GLP-1 RA to guideline pharmacotherapy was associated with a 43% relative reduction in all-cause mortality and a 47% reduction in hospitalization over three years. Significant decreases were also observed in AKI, atrial arrhythmias, AMI, and progression to dialysis, while ED visits increased. These findings support incorporating GLP-1 RAs into comprehensive HFpEF management and underline the need to clarify mechanisms driving emergency HF visits.
Khan, Zainab Zaib
(
University of Missouri-Columbia
, Columbia , Missouri , United States )
Khan, Aoun Zaib
(
MetroHealth
, Cleveland , Ohio , United States )
Sajid, Ahmed
(
PIMS, islamabad
, Islamabad , Pakistan )
Abdullah, Muhammad
(
HITEC Institute of Medical Sciences
, Taxilla , Pakistan )
Khan, Farva Zaib
(
ANMC
, Islamabad , Pakistan )
Khan, Mahnoor
(
Rashid Latif Medical College
, Lahore , Pakistan )
Author Disclosures:
Zainab Zaib Khan:DO NOT have relevant financial relationships
| Aoun Zaib Khan:DO NOT have relevant financial relationships
| Ahmed Sajid:DO NOT have relevant financial relationships
| Muhammad Huzaifa Ahsan:DO NOT have relevant financial relationships
| Muhammad Abdullah:DO NOT have relevant financial relationships
| Farva Zaib Khan:No Answer
| Mahnoor Khan:DO NOT have relevant financial relationships