Impella Use in AMI-Related Cardiogenic Shock is Associated with Increased Mortality and Complications Compared to Intra-Aortic Balloon Pump: A Propensity-Matched Real-World Analysis
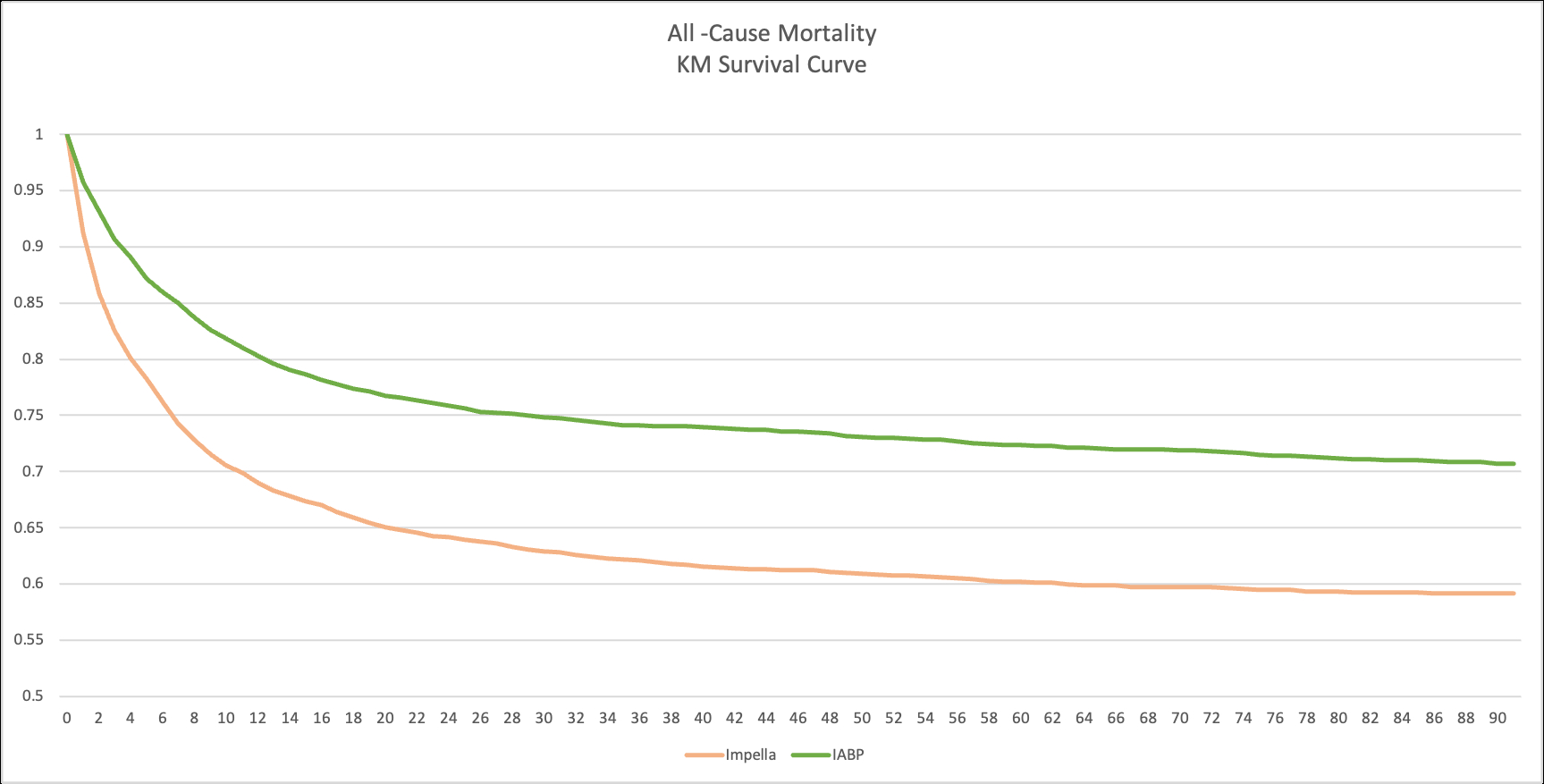
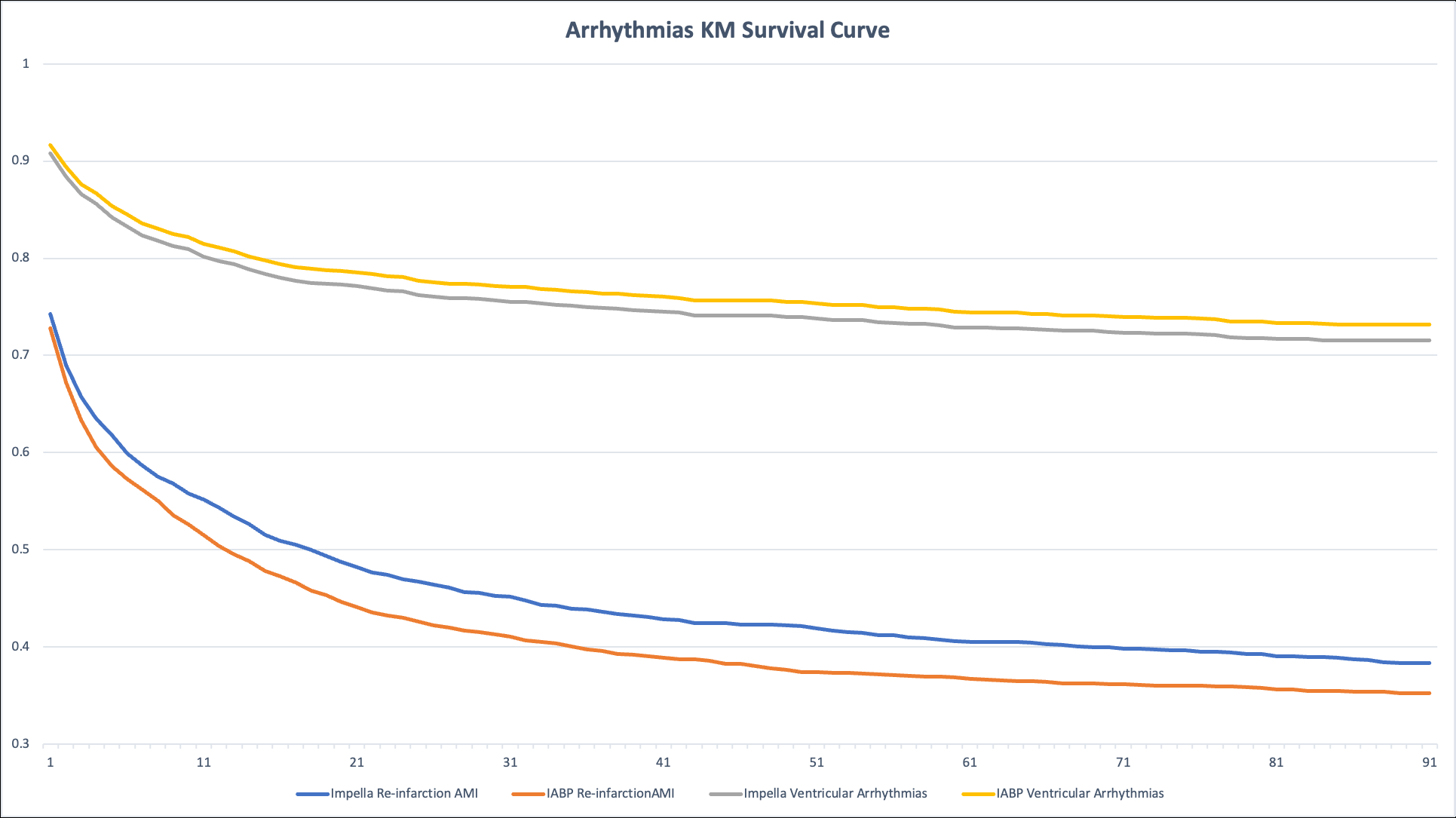
Abstract Body (Do not enter title and authors here): Background Mechanical circulatory support is often employed in acute myocardial infarction (AMI) complicated by cardiogenic shock. While Impella and IABP are widely used, real-world data comparing their safety and effectiveness remain limited. Research Question Does use of the Impella (axial-flow percutaneous ventricular assist device) device in AMI-related cardiogenic shock result in improved or worsened clinical outcomes compared to IABP (intra-aortic balloon pump)? Methods We conducted a retrospective cohort study using the TriNetX US Collaborative Network including adult patients (≥18 years) with AMI and cardiogenic shock between January 1, 2018, and January 1, 2025. Patients were categorized based on the receipt of Impella (n=3,787) or IABP (n=3,787) within one month of AMI diagnosis. Propensity score matching (1:1) was applied to balance baseline characteristics. The primary outcome was 90-day all-cause mortality. Secondary outcomes included ischemic stroke, intracranial bleeding, reinfarction, ventricular arrhythmias, sepsis, GI bleeding, device-related embolization, acute kidney injury, and limb ischemia. Statistical analyses included risk difference (RD), risk ratio (RR), hazard ratio (HR), and log-rank p-values for survival. Results Following matching, mean age was 70 years and 69% were male in both cohorts. Impella was associated with significantly higher mortality (36.7% vs 27.2%; RD +9.5% [95% CI 7.4–11.6], p<0.001; RR 1.35 [1.26–1.44]; HR 1.57 [1.45–1.71], p<0.001). Impella use also resulted in higher risk of intracranial bleeding (1.3% vs 0.7%; RD +0.6% [0.2–1.1], p=0.006; RR 1.92 [1.20–3.08]; HR 2.16 [1.34–3.46], p=0.001), sepsis (11.7% vs 9.7%; RD +2.0% [0.6–3.4], p=0.005; RR 1.21 [1.06–1.38]; HR 1.37 [1.19–1.57], p<0.001), major GI bleeding (6.4% vs 5.7%; HR 1.27 [1.05–1.52], p=0.012), and acute kidney injury (35.9% vs 33.7%; HR 1.21 [1.12–1.30], p<0.001). Ventricular arrhythmias were also more frequent in the Impella group (22.9% vs 21.8%; HR 1.18 [1.07–1.30], p=0.001). There were no significant differences in ischemic stroke, device-related embolization, or limb ischemia. Conclusion In AMI complicated by cardiogenic shock, Impella use was associated with increased 90-day mortality and higher incidence of intracranial bleeding, sepsis, and renal injury compared to IABP. These findings support cautious application of Impella in this high-risk population and highlight the need for further prospective trials.
Kaddour Hocine, Fouad
(
Bronxcare health system
, Bronx , New York , United States )
Khan, Zainab Zaib
(
University of Missouri
, Columbia , Missouri , United States )
Tilokani, Hersh
(
University of California
, Los Angeles , California , United States )
Khan, Farva Zaib
(
Al Nafees Medical College
, Islamabad , Federal , Pakistan )
Khan, Aoun Zaib
(
MetroHealth
, Cleveland , Ohio , United States )
Sajid, Ahmed
(
PIMS, islamabad
, Islamabad , Pakistan )
Yu, Serena
(
MetroHealth
, Cleveland , Ohio , United States )
Author Disclosures:
Fouad Kaddour Hocine:DO NOT have relevant financial relationships
| Zainab Zaib Khan:DO NOT have relevant financial relationships
| Hersh Tilokani:DO NOT have relevant financial relationships
| Farva Zaib Khan:No Answer
| Aoun Zaib Khan:DO NOT have relevant financial relationships
| Ahmed Sajid:DO NOT have relevant financial relationships
| Serena Yu:No Answer