Performance of Clinician-Assigned SCAI Shock Staging in the AHA Cardiogenic Shock Registry
Abstract Body (Do not enter title and authors here): Background: SCAI staging of cardiogenic shock (CS) severity facilitates communication about the presentation and trajectory of CS. Most prior validations of SCAI staging have used registry-specific algorithmic adaptations of the staging criteria. Few studies have evaluated clinician-assigned SCAI staging based on holistic assessment of all clinical data.
Aim: To assess the ability of initial and serial clinician-assigned SCAI staging to stratify risk of in-hospital mortality in a large, broadly representative CS population from the AHA CS Registry.
Methods: Consecutive CS admissions enrolled in the Registry (64 sites, 2022-2024) were included. Clinician-assigned SCAI stage was captured at CS onset (first 6h) and serially (6-12h after CS onset). Cases with available SCAI stage at both timepoints were classified as having improved, unchanged, or worsened SCAI stage. Associations of in-hospital mortality with initial and early change in SCAI stage were assessed using logistic regression; for the latter, models were adjusted for initial SCAI stage. Key subgroups defined by CS etiology (AMI-CS vs. HF-CS) and preceding cardiac arrest (CA) were examined.
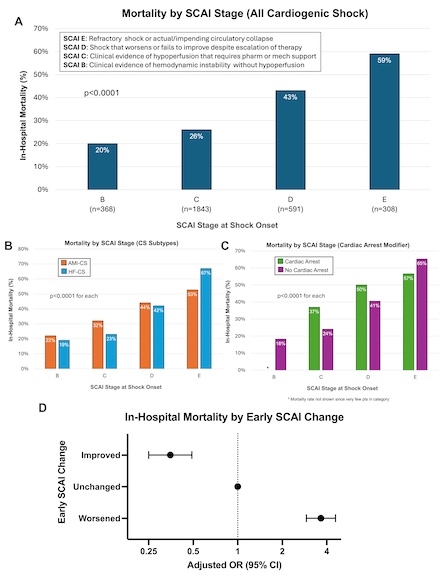
Results: Among 4,311 CS admissions, 3,110 (72%) had initial SCAI stage assessments (median age 66y, 33% women, 30% AMI-CS, 50% HF-CS, 21% preceding CA) and 2,867 (67%) had serial assessments. Most CS was initially staged as SCAI C (B: 12%; C: 59%; D: 19%; E: 10%), with a higher proportion of SCAI D/E in those with AMI-CS (34%) or preceding CA (60%). There was a stepwise gradient of mortality across SCAI stages (p<0.001; Fig-A), consistent when stratifying by CS etiology and preceding CA (p<0.001 for each; Fig-B/C). In the 12h after CS onset, most SCAI staging was unchanged (73%; worsening: 15%; improving: 12%); however, SCAI staging was more dynamic in those with preceding CA. Early worsening or improvement in SCAI stage was associated with higher (aOR 3.7, 95% CI 2.9-4.6) and lower (aOR 0.4, 95% CI 0.3-0.5) odds of mortality, respectively (Fig-D).
Conclusion: In this initial analysis from the AHA CS Registry, clinician-assigned SCAI staging effectively stratified in-hospital mortality risk, and early changes in SCAI stage further refined prognostication in CS.
Berg, David
(
Brigham and Women's Hospital TIMI Study Group
, Melrose , Massachusetts , United States )
Bohula, Erin
(
Brigham and Women's Hospital TIMI Study Group
, Melrose , Massachusetts , United States )
Patel, Siddharth
(
Brigham and Women's Hospital TIMI Study Group
, Melrose , Massachusetts , United States )
Palazzolo, Michael
(
Brigham and Women's Hospital TIMI Study Group
, Melrose , Massachusetts , United States )
Krucoff, Mitchell
(
DUKE MEDICAL CENTER
, Chapel Hill , North Carolina , United States )
Morrow, David
(
Brigham and Women's Hospital TIMI Study Group
, Melrose , Massachusetts , United States )
Author Disclosures:
David Berg:DO NOT have relevant financial relationships
| Erin Bohula:No Answer
| Siddharth Patel:DO have relevant financial relationships
;
Consultant:Janssen:Active (exists now)
| Michael Palazzolo:DO NOT have relevant financial relationships
| Mitchell Krucoff:DO have relevant financial relationships
;
Consultant:Gettinge:Active (exists now)
; Consultant:Boston Scientific:Past (completed)
; Consultant:Medtronic:Past (completed)
; Consultant:Abbott Vascular:Active (exists now)
; Consultant:Abiomed/J&J Medtech:Active (exists now)
; Consultant:Teleflex:Active (exists now)
| David Morrow:No Answer