Comparison of Clinical Risk Calculators for Atherosclerotic Cardiovascular Diseases: PREVENT, Pooled Cohort Equations, and QRISK3
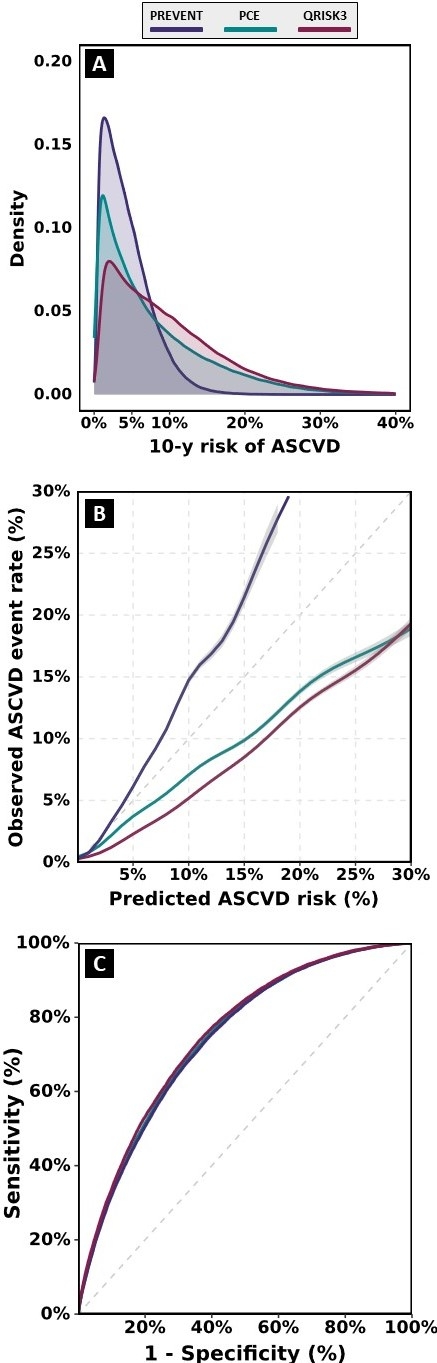
Abstract Body (Do not enter title and authors here): Introduction: The cardio-kidney-metabolic pathway has a crucial role in ASCVD, motivating development of the PREVENT equation. There is a need for external validation of the PREVENT equation and assessment of its performance in independent cohorts to assess generalizability across diverse populations. Aim: To compare predictive performance of the PREVENT equation with previously developed risk calculators; pooled cohort equations (PCE), and QRISK3. Methods: We used data from 500k participants of the United Kingdom Biobank (UKB). ASCVD was defined as the composite outcome of fatal and non-fatal myocardial infarction, coronary revascularization, and stroke. We ascertained demographic and clinical covariates required to calculate ASCVD risk, using the base model of PREVENT, PCE, and QRISK3, at the time of recruitment. Those with a diagnosis of ASCVD at the time of recruitment or missing data on age, sex, or ethnicity were excluded. We used the area under the ROC curve (AUC) and calibration plots for analysis. Results: Of 459,681 participants (mean age 56.3±8.1 years, 44.4% male, and 94.7% White), 24,514 (5.4%) participants had a new diagnosis of ASCVD during a 10-year follow-up. The median [interquartile range] of estimated 10-y ASCVD risk was 3.7% [1.9% - 6.1%] for PREVENT, 5.6% [2.4% - 11.3%] for PCE, and 8.0% [3.9% - 13.8%] for QRISK3 (Figure 1A). The calibration slope (95% CI) was 1.71 (1.66 – 1.76) for PREVENT, 0.64 (0.63 – 0.66) for PCE, and 0.66 (0.64 – 0.67) for QRISK3 (Figure 1B). The AUC for ASCVD prediction was 0.741 (0.738 - 0.744) for PREVENT, 0.744 (0.741 – 0.747) for PCE, and 0.751 (0.749 – 0.755) for QRISK3 (Figure 1C). Conclusion: In the UKB cohort, the PREVENT equation underpredicted while the PCE and QRISK3 overpredicted ASCVD risk, with a similar discrimination. Consequently, fewer individuals would be eligible for primary prevention with statins, based on the actionable thresholds of 7.5% or 10% when considering ASCVD risk based on PREVENT. Therefore, the external application of the PREVENT equation requires recalibration and context-specific interpretation.
Naderian, Mohammadreza
(
Mayo Clinic in Rochester
, Rochester , Minnesota , United States )
Kullo, Iftikhar
(
MAYO CLINIC
, Rochester , Minnesota , United States )
Author Disclosures:
Mohammadreza Naderian:DO NOT have relevant financial relationships
| Iftikhar Kullo:DO NOT have relevant financial relationships