A Polygenic Score to Identify Risk of Incident Stroke and Benefit from Primary Prevention Statin Therapy
Abstract Body (Do not enter title and authors here): Background: Primary prevention statin use has been shown to significantly reduce the incidence of stroke, however, clinical risk scores for statin eligibility do not predict stroke specifically. A polygenic risk score (PRS) for stroke is a tool that may help identify individuals at greatest risk of stroke and most likely to benefit from statin therapy.
Methods: We performed a prospective cohort study using genotyped individuals from a large primary prevention RCT (JUPITER), which tested rosuvastatin 20 mg daily vs placebo. We applied the validated GIGASTROKE PRS categorized by quintiles: low (Q1), moderate (Q2-Q4) or high risk (Q5). The primary outcome was occurrence of all-cause stroke. PRS risk was modeled per 1-SD and hazard ratios calculated for the moderate and high-risk groups relative to low risk. Formal testing of treatment interaction for rosuvastatin and PRS was performed.
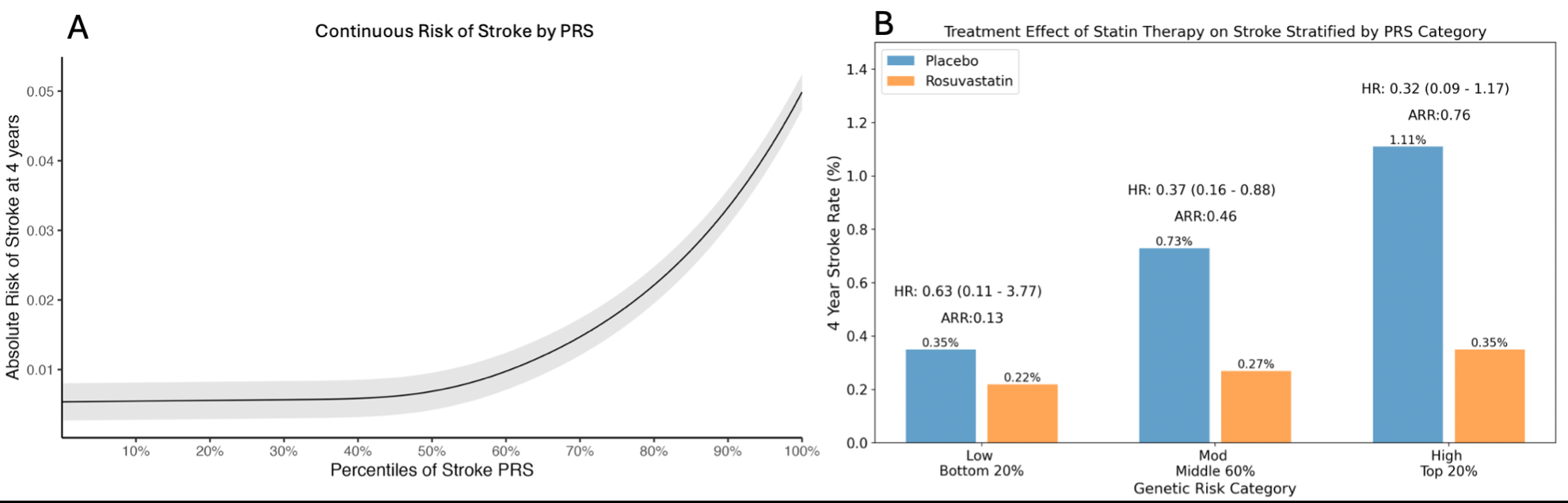
Results: Of 8,749 patients with genetic data (32% male, mean age 66), the median LDL-C was 110 mg/dL and hsCRP was 4.05 mg/L. During 4 years of follow up, 44 patients suffered a stroke. The PRS was strongly associated with risk of incident stroke (Fig, A). Compared to those at low genetic risk, the absolute risk of stroke was more than 2-fold greater in the moderate group (HR: 2.10, 0.78-5.67) and nearly 4-fold greater in the high-risk group (HR: 3.72, 1.27-10.88, p-trend =0.011). In this genetic cohort, rosuvastatin reduced the risk of stroke by 61% (HR: 0.39, 0.20-0.76, p=0.006). The relative risk reductions with rosuvastatin were 37% (HR 0.63, 0.11-3.77), 63% (HR 0.37, 0.16-0.88), and 68% (HR 0.32, 0.09-1.17) in low, moderate, and high-risk groups, respectively. The absolute risk reductions with rosuvastatin were 0.13% (-0.38-0.63), 0.46% (0.08-0.84), and 0.76% (-0.03-1.56) (Fig, B). Rosuvastatin in the high-risk subgroup reduced the incidence of stroke to the level of the low-risk subgroup receiving placebo (0.35%).
Conclusion: A PRS can identify primary prevention patients with a 2 to 4-fold increased risk of stroke, which appears to be largely offset with statin therapy. As the use of PRSs increase in clinical practice, it may be a useful tool to help guide statin initiation for primary stroke prevention.
Mcclintick, Daniel
(
Brigham and Womens Hospital
, Boston , Massachusetts , United States )
Kamanu, Frederick
(
Brigham and Womens Hospital
, Boston , Massachusetts , United States )
Melloni, Giorgio
(
Brigham and Women's Hospital
, Boston , Massachusetts , United States )
Sabatine, Marc
(
Brigham and Women's Hospital
, Boston , Massachusetts , United States )
Ruff, Christian
(
BRIGHAM WOMENS HOSPITAL
, Boston , Massachusetts , United States )
Ridker, Paul
(
BRIGHAM WOMENS HOSPITAL
, Boston , Massachusetts , United States )
Chasman, Daniel
(
Brigham and Women's Hospital
, Boston , Massachusetts , United States )
Marston, Nicholas
(
Brigham And Womens Hospital
, Boston , Massachusetts , United States )
Author Disclosures:
Daniel McClintick:DO NOT have relevant financial relationships
| Frederick Kamanu:No Answer
| Giorgio Melloni:DO NOT have relevant financial relationships
| Marc Sabatine:DO have relevant financial relationships
;
Research Funding (PI or named investigator):Amgen:Active (exists now)
; Research Funding (PI or named investigator):Pfizer:Active (exists now)
; Research Funding (PI or named investigator):Novartis:Active (exists now)
; Research Funding (PI or named investigator):Merck:Active (exists now)
; Research Funding (PI or named investigator):Ionis:Active (exists now)
; Consultant:AstraZeneca:Active (exists now)
; Individual Stocks/Stock Options:AstraZeneca:Active (exists now)
; Consultant:Anthos:Active (exists now)
; Research Funding (PI or named investigator):Anthos:Active (exists now)
; Consultant:Amgen:Active (exists now)
| Christian Ruff:DO NOT have relevant financial relationships
| Paul Ridker:DO have relevant financial relationships
;
Researcher:NovoNordisk:Active (exists now)
; Ownership Interest:Uppton, Bitteroot, Angiowave ,:Active (exists now)
; Consultant:NovoNordisk, Agepha, Ardelyx, Arrowhead, CSK Behring, SOCAR, Eli Lilly, New Amsterdam, cardio Therapeutics, Uppton:Active (exists now)
; Researcher:NHLBI:Active (exists now)
; Researcher:Pfizer:Active (exists now)
; Researcher:Kowa:Active (exists now)
| Daniel Chasman:DO NOT have relevant financial relationships
| Nicholas Marston:DO have relevant financial relationships
;
Speaker:Amgen:Past (completed)
; Researcher:Pfizer:Past (completed)
; Consultant:NewAmsterdam:Past (completed)
; Researcher:Marea:Active (exists now)
; Researcher:Ionis:Active (exists now)
; Researcher:Amgen:Active (exists now)