Ventricular Tachycardia Mortality Trends in Oncology: Where Are We Now?
Abstract Body (Do not enter title and authors here): Background Advancements in chemotherapeutic modalities lead to improved cancer survival rates. While the cardiotoxicity related to the therapies is increasingly recognized, real-world data on ventricular tachycardia (VT) mortality among them is limited.
Objective This study sought to determine the longitudinal cardiovascular mortality trends related to ventricular tachycardia in the cancer population.
Methods We queried the CDC WONDER database among patients ≥ 25 years old from 1999 to 2020. Cardiovascular disease was listed as the main cause of death, while VT and cancer were listed as contributing causes of death. We calculated age-adjusted mortality rates (AAMR) per 1,000,000 individuals. We determined the trends over time by estimating the annual percent change (APC) using the Joinpoint regression program.
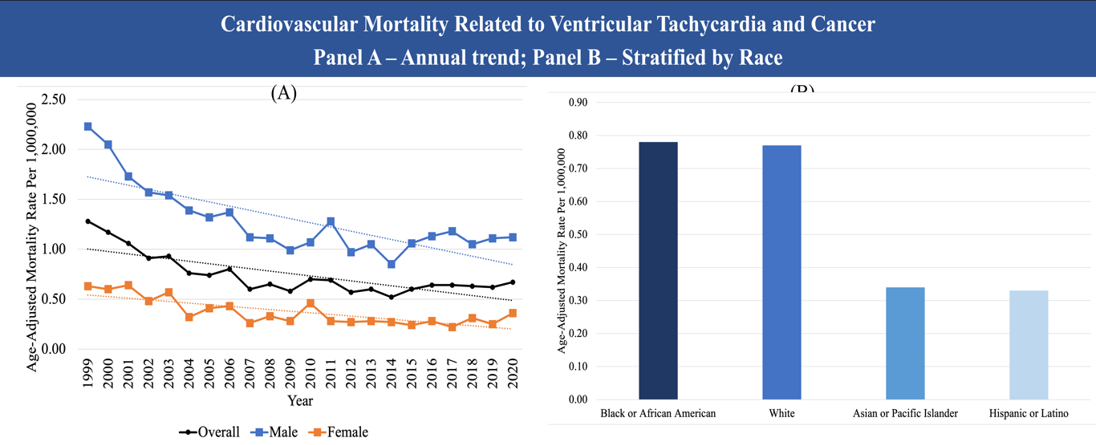
Results In the study period, there were 3,483 cardiovascular mortalities related to ventricular tachycardia in patients with comorbid cancer. The overall AAMR decreased significantly from 1.28 (95% CI, 1.11-1.44) in 1999 to 0.67 (95% CI, 0.57- 0.77) in 2020, with an average APC of -2.91 (95% CI, -3.95, -1.86). Overall, males had higher AAMR than females (1.25 [95% CI, 1.20 – 1.30] vs. (0.36 [95% CI, 0.34 – 0.39]). African Americans and White patients have comparable AAMR of 0.78 (95% CI, 0.69-0.86) and 0.77 (95% CI, 0.74-0.80), respectively, which were higher than Asians (0.34 [95% CI, 0.25-0.44]) and Hispanics (0.33 [95% CI, 0.27-0.40]). The AAMR was higher in the rural region than in the urban region (0.72 [95% CI, 0.69 – 0.75] vs. 0.76 [95% CI, 0.70 – 0.81]). The West region had the highest AAMR (0.79 [95% CI, 0.74 – 0.85]).
Conclusion Cardiovascular mortality related to VT in patients with comorbid cancer dropped significantly throughout the years. Further targeted approaches are needed to address the disparities in sex, race, and region.
Yeo, Yong Hao
(
William Beaumont Hospital Royal Oak
, ROYAL OAK , Michigan , United States )
San, Boon Jian
(
Jacobi Medical Center/ Albert Einstein College of Medicine
, Bronx , New York , United States )
Tan, Min Choon
(
Saint Michael's Medical Center
, Newark , New Jersey , United States )
Ang, Qi Xuan
(
Sparrow Health System and Michigan State University
, East Lansing , Michigan , United States )
Lee, Justin
(
Cleveland Clinic
, Cleveland , Ohio , United States )
Mehta, Nishaki
(
William Beaumont Hospital
, Royal Oak , Michigan , United States )
Author Disclosures:
Yong Hao Yeo:DO NOT have relevant financial relationships
| Boon Jian San:DO NOT have relevant financial relationships
| Min Choon Tan:DO NOT have relevant financial relationships
| Qi Xuan Ang:DO have relevant financial relationships
;
Employee:University of Michigan Health Sparrow Hospital:Active (exists now)
| Justin Lee:DO have relevant financial relationships
;
Speaker:Boston Scientific:Past (completed)
| Nishaki Mehta:DO have relevant financial relationships
;
Speaker:medtronic:Past (completed)
; Speaker:abbott:Past (completed)
; Speaker:Boston scientific :Past (completed)