Clinical Outcomes of Myocardial Infarction with Non-Obstructive Coronary Arteries in Patients with Prior Irradiation History
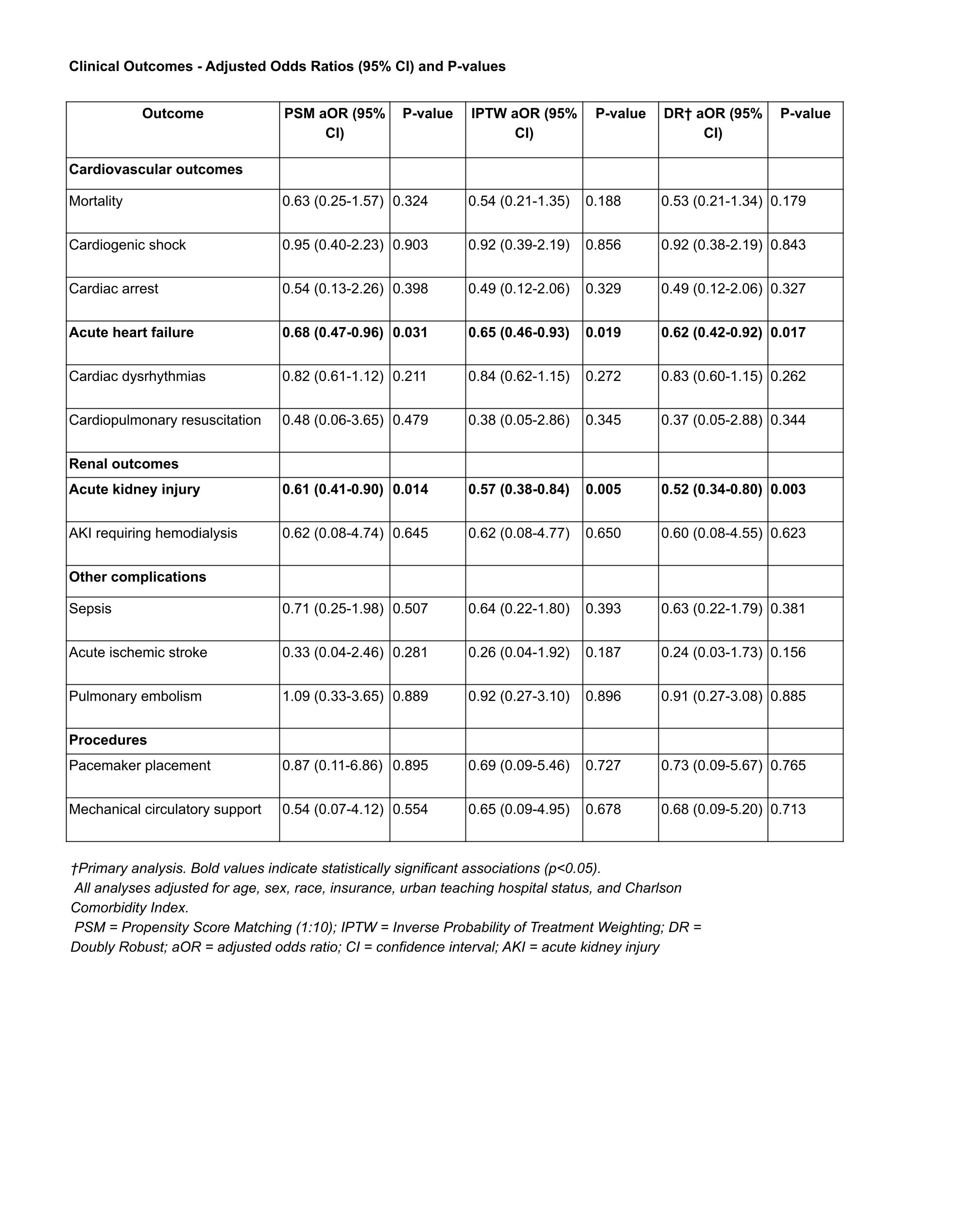
Abstract Body: Background: Thoracic radiation therapy is associated with accelerated atherosclerosis and microvascular dysfunction that may manifest years after exposure. While radiation-induced coronary disease typically involves epicardial vessels, its impact on myocardial infarction with non-obstructive coronary arteries (MINOCA) remains poorly defined. We evaluated in-hospital outcomes among MINOCA patients with a prior history of irradiation. Methods: Adults with MINOCA were identified from the National Inpatient Sample (2017–2022) using validated ICD-10 algorithms. Patients with a personal history of irradiation were compared with controls without active or prior cancer. To reduce confounding, three analytic approaches were used: propensity score matching (PSM; 1:10 nearest neighbor, 0.2 SD caliper), inverse probability of treatment weighting (IPTW with stabilized weights), and doubly robust (DR) estimation. Propensity scores included age, sex, race, Medicare status, urban teaching hospital status, and the Charlson Comorbidity Index. All analyses accounted for the complex survey design. Results: We identified 1,075 patients with prior irradiation and 71,540 controls. PSM yielded 1,075 exposed patients matched to 9,360 unexposed controls. IPTW and DR methods achieved superior covariate balance compared with PSM. In DR models, prior irradiation was independently associated with lower odds of acute kidney injury (aOR 0.52, 95% CI 0.34–0.80, p=0.003) and acute heart failure (aOR 0.62, 95% CI 0.42–0.92, p=0.017). Results were consistent across PSM and IPTW analyses. No significant associations were observed for in-hospital mortality, cardiac arrest, cardiogenic shock, ischemic stroke, arrhythmias, dialysis, mechanical circulatory support, pacemaker implantation, or pulmonary embolism. Conclusions: In this national cohort of MINOCA hospitalizations, prior irradiation was paradoxically associated with lower odds of acute kidney injury and acute heart failure. These findings may reflect survivor bias, management differences, or unmeasured confounding and warrant further investigation to clarify mechanisms and implications for risk stratification.
Bin Firos, Juma
(
Trinity Health Livonia Hospital
, Livonia , Michigan , United States )
Anamika, Fnu
(
Cleveland Clinic Akron General
, Akron , Ohio , United States )
Dixit, Sakshi
(
Cleveland Clinic Akron General
, Akron , Ohio , United States )
Kumar, Nomesh
(
OSF Saint Francis Medical Center
, Peoria , Illinois , United States )
Author Disclosures:
Juma Bin Firos:DO NOT have relevant financial relationships
| FNU Anamika:No Answer
| Sakshi Dixit:No Answer
| Kamleshun Ramphul:DO NOT have relevant financial relationships
| Nomesh Kumar:No Answer