The contribution of morbidity clusters in late life to stroke incidence and severity: The Atherosclerosis Risk in Communities (ARIC) study
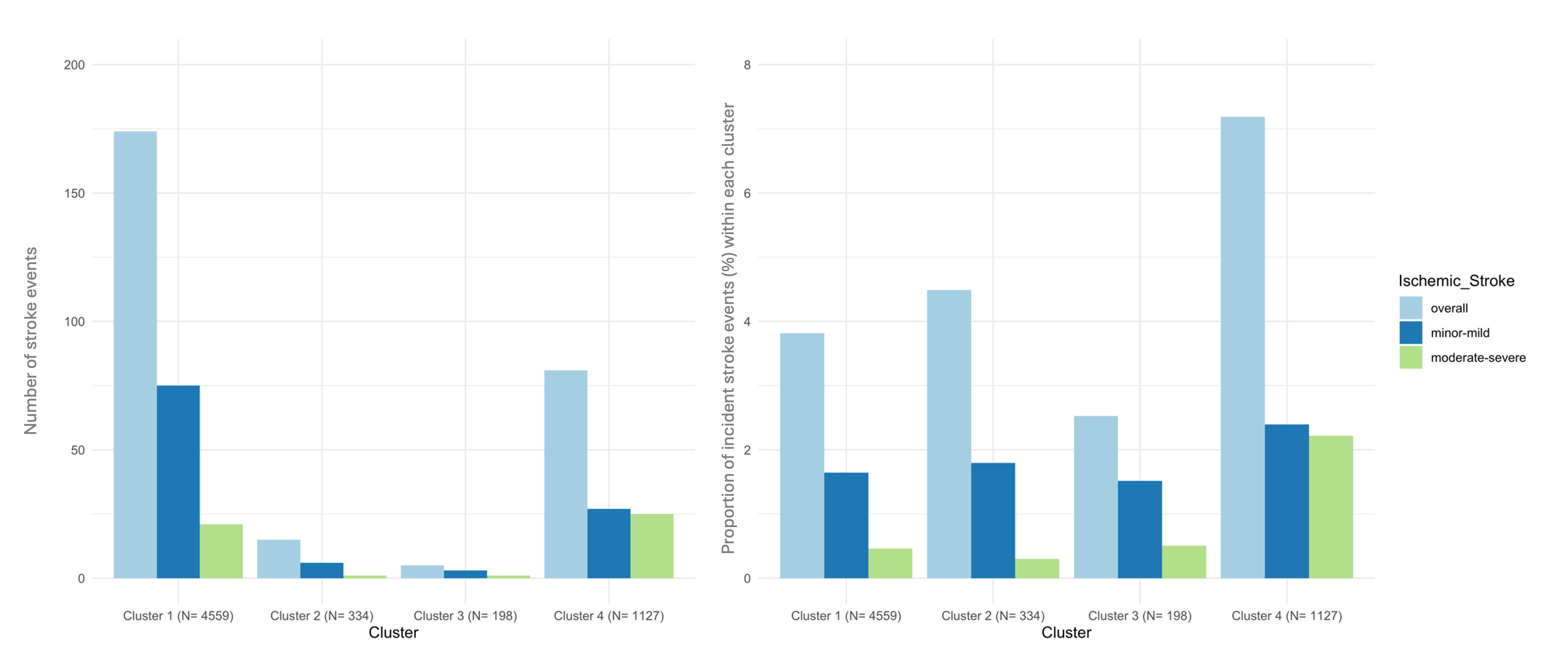
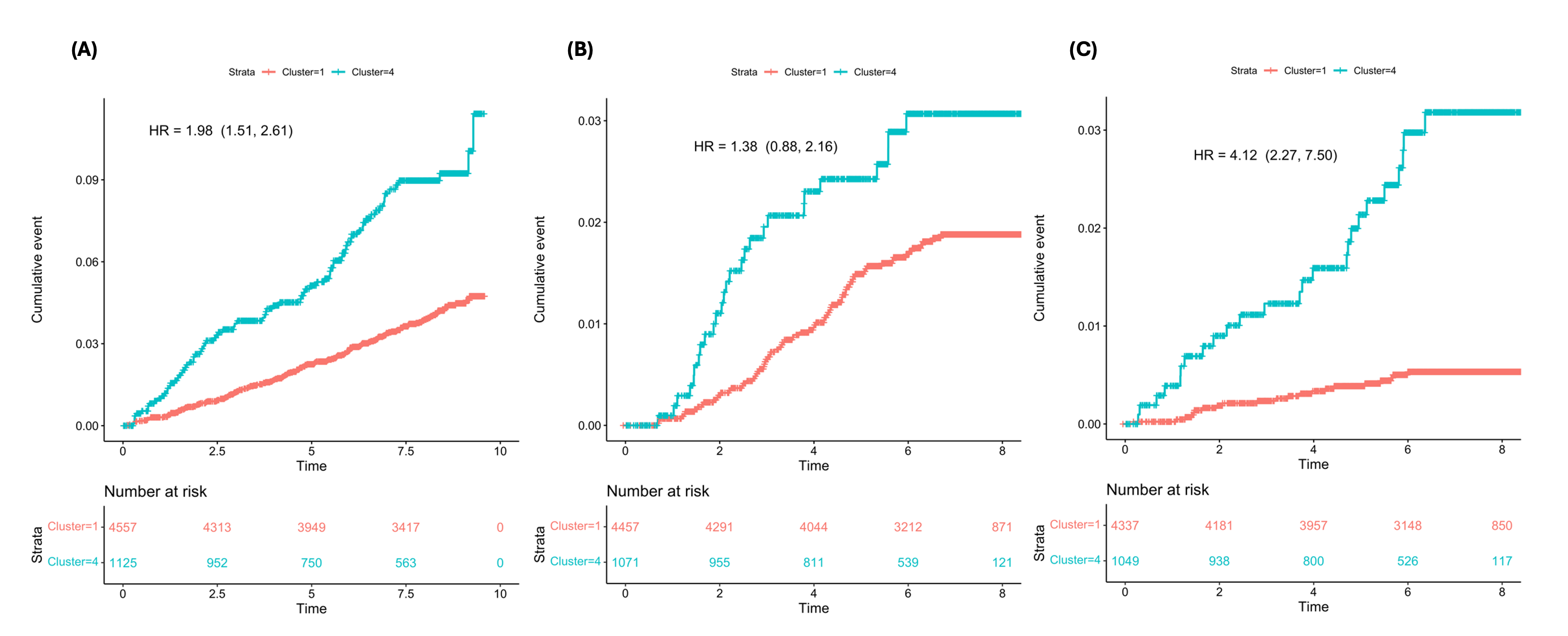
Abstract Body: Objective: Vascular risk factors significantly increase the risk of stroke, but it is unclear how to best assess the overall morbidity burden. In our previous work, a cluster analysis successfully grouped individuals into clusters based on similar clinical profiles in midlife and showed differences in 30-year stroke outcomes across clusters. The current study explores whether clinically meaningful clusters of morbidities can also be derived in older age, when morbidity burden is overall higher, and whether clusters based on late-life risk factors predict stroke incidence and severity. Methods: Participants seen at visit 5 of the ARIC study (2011-2013; N= 6218, median age 75, 59% female, 23% Black) without prevalent stroke were included. Employing an unsupervised agglomerative hierarchical clustering approach, participants were allocated into clusters based on late-life clinical information and they were followed for incident stroke through 2020. Standard criteria were used to assign defining features to each cluster. The association between the clusters and overall ischemic stroke incidence (and with ischemic stroke incidence stratified by stroke severity (minor-mild stroke: NIHSS≤5; moderate-severe stroke: NIHSS>5), was assessed using a Cox regression model with Firth bias correction, adjusted for age, sex, education, and race-center. Results: Of the 275 incident ischemic strokes diagnosed between visit 5 and 2020, 159 had NIHSS grading. Four late-life clusters were identified, with the following defining features: cluster 1 (relatively healthy); cluster 2 (smoking); cluster 3 (cancer); cluster 4 (heart failure, coronary heart disease, diabetes, atrial fibrillation, peripheral artery disease, renal dysfunction, and late-life depression). Due to a very low stroke incidence, cluster 2 (N= 15) and 3 (N= 5) were excluded from the time-to event analysis (Figure 1). Individuals in cluster 4 compared to cluster 1 had a significantly greater stroke risk (HR(95%CI)= 1.98 (1.51, 2.61)) (Figure 2). The association of cluster 4 vs. cluster 1 remained significant for moderate-severe stroke (vs. no stroke) (HR(95%CI)= 4.12 (2.27, 7.50)), but not for minor-mild stroke (vs. no stroke) (HR(95%CI)= 1.38 (0.88, 2.16)). Conclusion: Morbidity clusters in late life can be used to predict stroke incidence and severity. Cluster analysis is a valuable approach to capture morbidity and stroke-related disability in late-life.
Egle, Marco
(
NINDS
, Bethesda , Maryland , United States )
Groechel, Renee
(
NINDS
, Bethesda , Maryland , United States )
Johansen, Michelle
(
JOHNS HOPKINS HOSPITAL
, Baltimore , Maryland , United States )
Kucharska-newton, Anna
(
UNIVERSITY NORTH CAROLINA
, Chapel Hill , North Carolina , United States )
Gottesman, Rebecca
(
NINDS
, Bethesda , Maryland , United States )
Koton, Silvia
(
TEL AVIV UNIVERSITY
, Tel Aviv , Israel )
Author Disclosures:
Marco Egle:DO NOT have relevant financial relationships
| Renee Groechel:DO NOT have relevant financial relationships
| Michelle Johansen:DO NOT have relevant financial relationships
| Anna Kucharska-Newton:DO NOT have relevant financial relationships
| Rebecca Gottesman:DO NOT have relevant financial relationships
| Silvia Koton:DO NOT have relevant financial relationships