Disparities in the utilization of inpatient rehabilitation facilities for stroke patients in the United States
Abstract Body: Background We evaluate the contemporary trends and socioeconomic disparities in utilization of post-stroke rehabilitation using statewide inpatient data from 5 states with large and diverse populations.
Methods We used ICD codes (I60, I61, I63) to identify adult patients (≥18 years) discharged home (including home health), to IRF, or skilled nursing facility (SNF) with acute ischemic stroke (AIS), spontaneous intracerebral hemorrhage (ICH), or subarachnoid hemorrhage (SAH) primary diagnosis from the inpatient databases of Florida, Georgia, Maryland, New York, and Washington (2016-2019). Utilizing multivariable logistic regression multivariable logistic regression with patient-level cluster-robust standard errors, we evaluate the correlates of discharge to IRF (vs. home and SNF) and report the adjusted odds ratios (aOR) and 95% confidence intervals (CI).
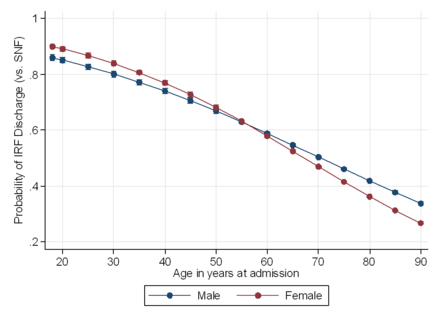
Results Overall, 335,521 stroke discharges (88.4% AIS, 8.1% ICH, 3.5% SAH) representing 312,316 unique patients (median age [IQR] of 69 [59-80] and 47.9% female) were included. Among these, 21.8% discharges were to IRF, 51.5% to home, and 26.7% to SNF. Between 2016 and 2019, the overall proportion of IRF discharges did not change significantly (21.8% in 2016; 22.1% in 2019). Patients with ICH (vs. AIS) were more likely to be discharged to IRF (vs. home) (aOR, CI: 2.17, 2.10-2.26). Patients discharged to IRF (vs. SNF) were more likely to be privately (vs. Medicare) insured (1.73, 1.66-1.79), and reside in the highest income quartile zip codes, vs. lowest quartile (aOR, CI: 1.31, 1.26-1.35). Conversely, non-Hispanic Black (vs. non-Hispanic White individuals were less likely to be discharged to IRF (vs. SNF) (aOR, CI: 0.92, 0.89 – 0.94). Stroke patients with higher comorbidity burden, as measured by Charlson Comorbidity Index (aOR, CI: 0.88, 0.87-0.89), and those undergoing invasive ventilation (0.79, 0.75-0.83) and tracheostomy (0.35, 0.32-0.38) were also less likely to be discharged to IRF (vs. SNF). We observed an age-dependent association between sex and IRF discharge whereby older females (vs. males) are less likely to be discharged to IRF in lieu of SNF (p-value for interaction <0.001; Figure 1).
Conclusion Less than 1 in 4 stroke patients receive post-acute IRF care, highlighting a critical gap in achieving optimal stroke recovery. Furthermore, notable sociodemographic disparities persist in IRF utilization. Maximizing pathways for optimal post-stroke recovery remains a critical gap in stroke systems of care.
Bako, Abdulaziz
(
Houston Methodist
, Houston , Texas , United States )
Potter, Thomas
(
Houston Methodist
, Houston , Texas , United States )
Pan, Alan
(
Houston Methodist
, Houston , Texas , United States )
Borei, Karim
(
Houston Methodist
, Houston , Texas , United States )
Vahidy, Farhaan
(
TIRR Memorial Hermann
, Houston , Texas , United States )
Author Disclosures:
Abdulaziz Bako:DO NOT have relevant financial relationships
| Thomas Potter:DO NOT have relevant financial relationships
| Alan Pan:DO NOT have relevant financial relationships
| Karim Borei:DO NOT have relevant financial relationships
| Farhaan Vahidy:DO NOT have relevant financial relationships