Readmission to Acute Care from Inpatient Rehabilitation Among Patients with Acute Ischemic Stroke
Abstract Body: Introduction: Inpatient rehabilitation (IR) for patients with Acute Ischemic Stroke (AIS) offers improved functional recovery and quality of life. Readmission (RA) to acute care during IR may compromise this favorable recovery trajectory. We seek to define the factors associated discharge to IR, and RA from IR, after AIS.
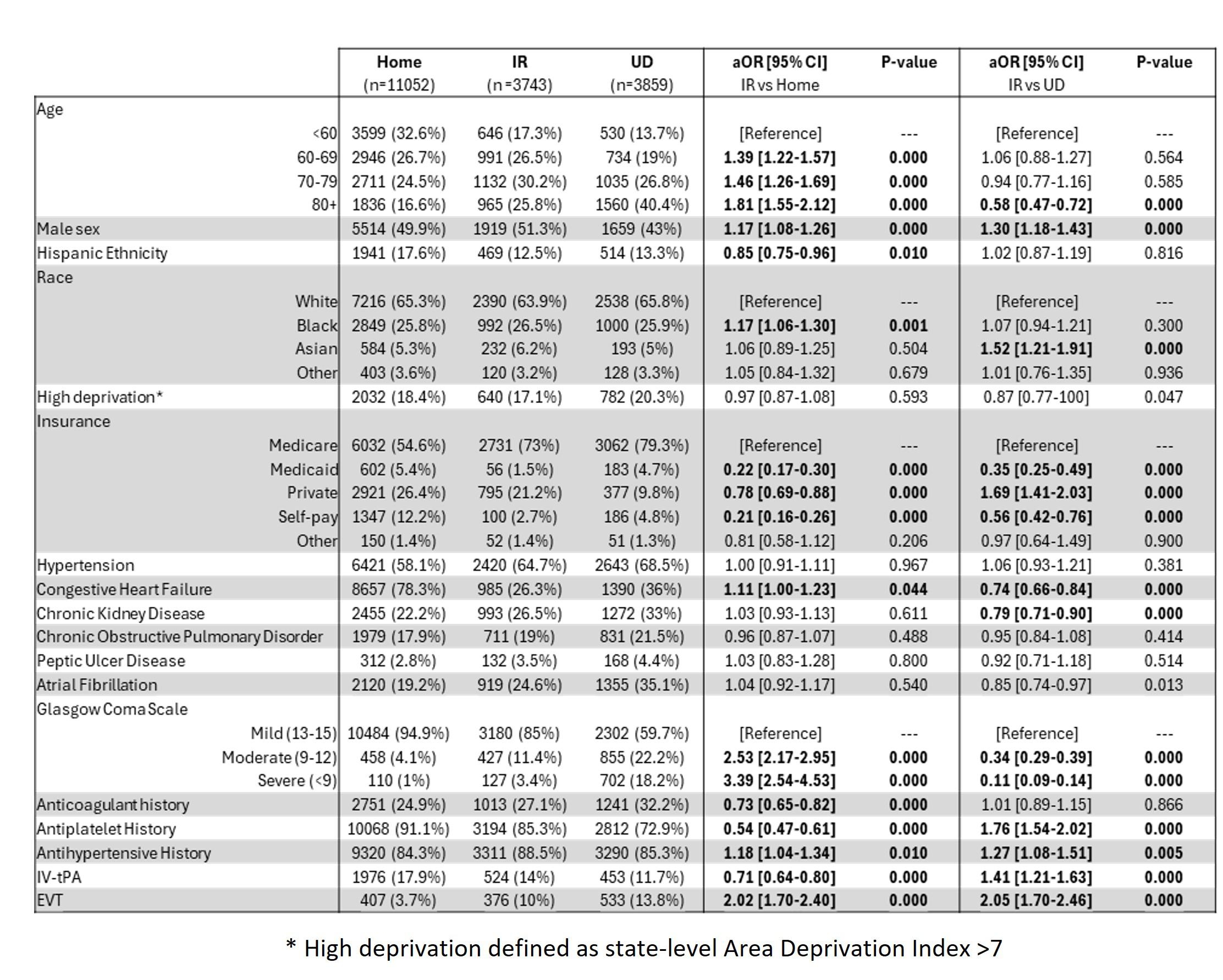
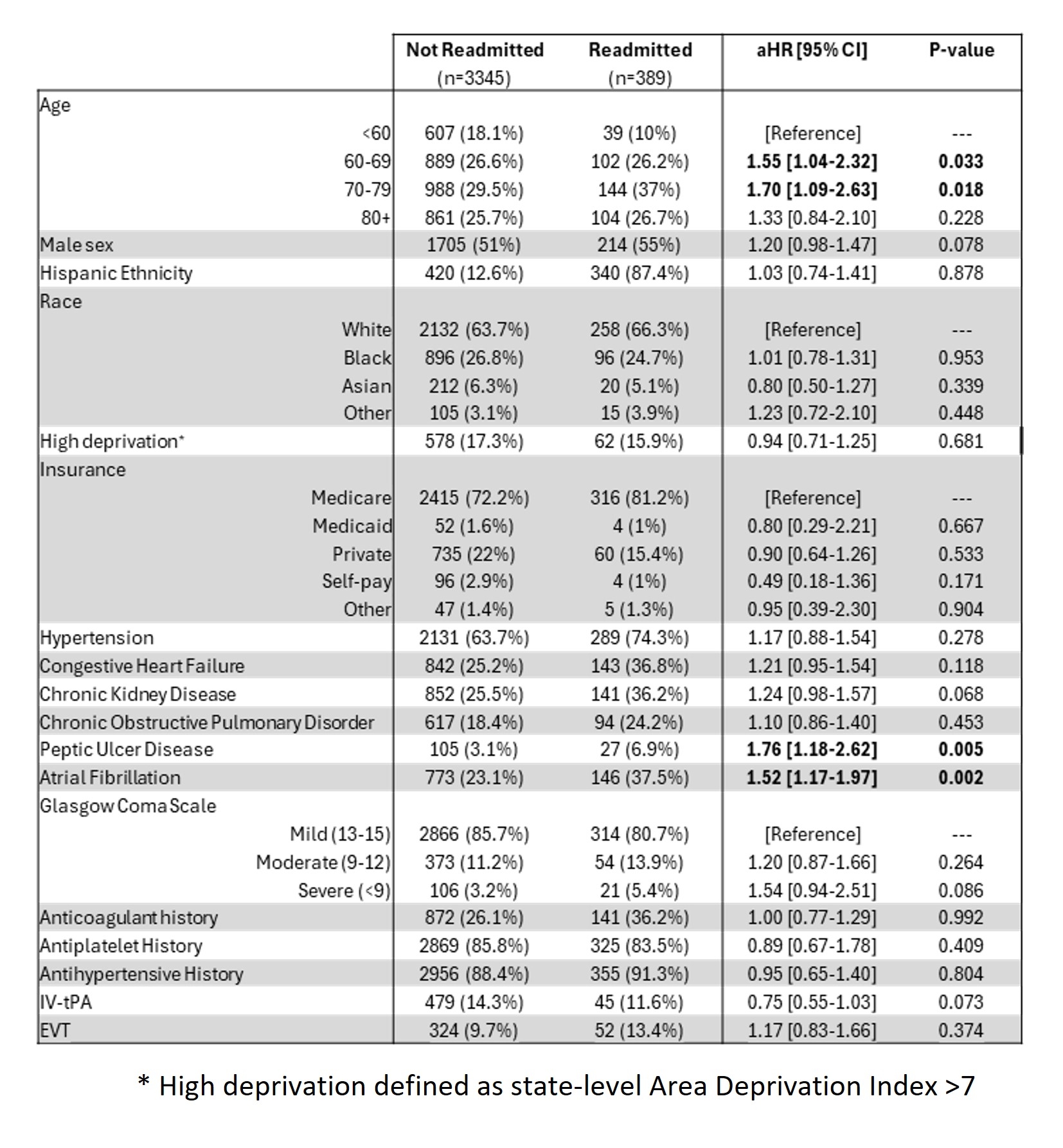
Methods: Data for adult (>18) AIS patients admitted from May 2016-May 2024 were retrieved from the Registry of Neurological Endpoint Assessment among Patients with Ischemic and Hemorrhagic Stroke (REINAH), including demographics, comorbidities, clinical scores, use of endovascular thrombectomy (EVT) and intravenous tissue plasminogen activator (IV-tPA), and discharge dispositions. Separate multivariable logistic regression models were fit to determine factors associated with discharge to IR vs. home (model 1) and IR vs. unfavorable discharge (UD; long-term acute care, skilled nursing facility, hospice, expired, other; model 2). Adjusted odds ratios (aOR) and 95% confidence intervals (CI) are reported. Cox proportional hazard models were fit to determine the hazard of 30-day RA for patients discharged to IR, with adjusted hazard ratios (aHR) and 95% CI reported.
Results: A total of 18,645 AIS patients were included, comprising 51.2% female and15.7% Hispanic patients with a racial distribution of 65.1% White, 26.0% Black, 5.4% Asian, and 3.5% Other. A total of 3,743 (20.0%) patients discharged to IR, 11,052 (59.3%) discharged home, and 3859 (20.7%) had UD. Of patients discharged to IR, 389 (10.4%) readmitted within 30 days. Across both IR discharge models, patients who were male (aORs: 1.17 [1.08-1.26]; 1.30 [1.18-1.43]), [FV2] had a history of antihypertensive use (1.18 [1.04-1.34]; 1.27 [1.08-1.51]), and received EVT (2.02 [1.70-2.40]; 2.05 [1.70-2.46]) were more likely to discharge to IR (vs. home or UD) (Figure 1). Consequently, patients who were self-pay (vs. Medicare, 1.17 [1.08-1.26]; 1.30 [1.18-1.43]) or on Medicaid (1.17 [1.08-1.26]; 1.30 [1.18-1.43]) had lower odds of discharge to IR (vs. home or UD). Among patients discharged to IR, those aged 60-69 years (vs. < 60) (aHR: 1.55 [1.04-2.32]), 70-79 years (1.70 [1.09-2.63]), with peptic ulcer disease (1.76 [1.18-2.62]) and atrial fibrillation (1.52 [1.17-1.97]) had higher odds of RA (Figure 2). Discussion: Males and patients receiving EVT were more likely to discharge to IR, while those with peptic ulcer disease and atrial fibrillation who discharged to IR faced a greater risk of RA.
Potter, Thomas
(
Houston Methodist
, Houston , Texas , United States )
Borei, Karim
(
Houston Methodist
, Houston , Texas , United States )
Khan, Osman
(
Houston Methodist
, Houston , Texas , United States )
Bako, Abdulaziz
(
Houston Methodist
, Houston , Texas , United States )
Pan, Alan
(
Houston Methodist
, Houston , Texas , United States )
Vahidy, Farhaan
(
TIRR Memorial Hermann
, Houston , Texas , United States )
Author Disclosures:
Thomas Potter:DO NOT have relevant financial relationships
| Karim Borei:DO NOT have relevant financial relationships
| Osman Khan:No Answer
| Abdulaziz Bako:DO NOT have relevant financial relationships
| Alan Pan:DO NOT have relevant financial relationships
| Farhaan Vahidy:DO NOT have relevant financial relationships