Disparities in the surgical treatment of ruptured and unruptured brain arteriovenous malformation: a population-based study across 5 diverse US states
Abstract Body: Objectives
We evaluate the sociodemographic and clinical factors associated with receiving surgical AVM treatment and the likelihood of rupture using data from five states with large and diverse populations in the United States.
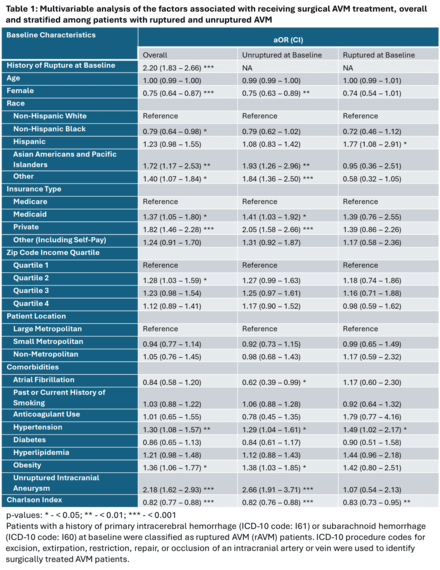
Methods: We used the ICD-10 code Q28.2 to identify patients with a diagnosis of AVM from the statewide inpatient and emergency department databases of Florida, Georgia, Maryland, New York, and Washington (2016-2019). Patients with a history of primary intracerebral hemorrhage or subarachnoid hemorrhage at baseline were classified as ruptured AVM (rAVM) patients. ICD-10 procedure codes were used to identify surgically treated AVM patients (Table 1). Multivariable logistic regression models were used to evaluate the sociodemographic and clinical factors associated with receiving craniotomy. A mixed-effects logistic model with patient-level random effects was used to identify the independent predictors of subsequent rupture. Adjusted odds ratios (aOR) and 95% confidence interval (CI) are reported.
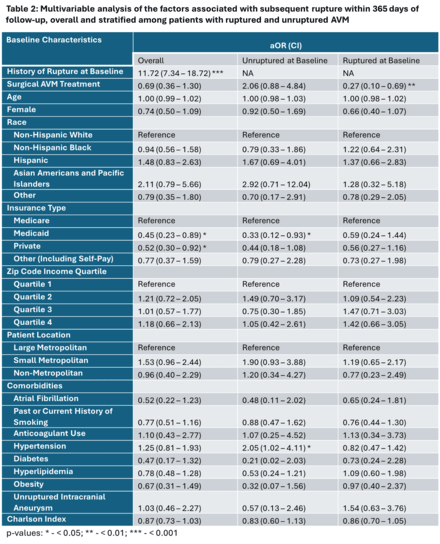
Results: Overall, 4,144 AVM patients (50.3% female; 54.5% non-Hispanic White [NHW]), with a median age (IQR) of 54 (38-67) were included, of which 761(18.4%) were rAVM patients, 1 016(24.5%) received surgical treatment (22.0% in unruptured and 35.7% in rAVM patients), and 161(3.9%) experienced subsequent rupture (2.0% in unruptured and 12.0% in rAVM patients). Non-Hispanic Black (NHB), vs. NHW patients (0.80, 0.64 – 0.99) and females (0.75, 0.64 -0.87) had lower odds of receiving surgical AVM treatment, whereas Asian (vs. NHW) patients (1.76, 1.20 – 2.58) and privately insured (vs. Medicare) patients (1.82, 1.45 – 2.26) had higher odds of receiving surgical AVM treatment (Table 1). Furthermore, rAVM patients were over 10 times more likely to experience a subsequent rupture (aOR, CI: 10.82, 6.95-16.83). Although surgical AVM treatment was not significantly associated with subsequent rupture in the overall AVM population 0.69 (0.36-1.30; Table 2), among patients with rAVM, surgical treatment was significantly associated with lower odds of subsequent rupture (0.29, 0.11-0.73).
Conclusion: Patients with ruptured AVM are over 10 times more likely to experience a subsequent rupture. Although surgical treatment significantly reduces the likelihood of subsequent rupture among ruptured AVM patients, sociodemographic disparities in receiving surgical treatment persist. Further research is warranted to address these inequities and improve outcomes.
Bako, Abdulaziz
(
Houston Methodist
, Houston , Texas , United States )
Khan, Osman
(
Houston Methodist
, Houston , Texas , United States )
Britz, Gavin
(
Houston Methodist Hospital
, Houston , Texas , United States )
Author Disclosures:
Abdulaziz Bako:DO NOT have relevant financial relationships
| Osman Khan:No Answer
| Gavin Britz:DO NOT have relevant financial relationships