Risk of Recurrent Ischemic Stroke Among Patients with Cryptogenic Stroke and Left Ventricular Ejection Fraction
Abstract Body: BACKGROUND: Nearly one-quarter of ischemic strokes (IS) in the U.S. are recurrent. We aimed to determine the risk of recurrent IS associated with reduced left ventricular ejection fraction (LVEF) in patients enrolled in the ARCADIA trial.
METHODS: We performed a post-hoc exploratory analysis in the ARCADIA trial, a phase III RCT of 1,015 cryptogenic stroke patients with atrial cardiopathy from February 2018 to February 2023. Those with LVEF <30% were not eligible. We dichotomized patients with LVEF into <50% and >50% and built adjusted Cox proportional hazard models to estimate the hazard ratio (HR) of recurrent IS within each LVEF strata by treatment strategy of apixaban versus aspirin. Significance of the interaction was assessed after adjustment for imbalanced covariates found among these groups.
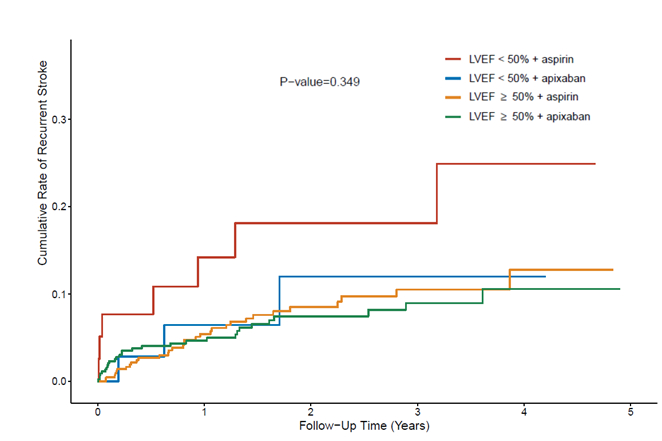
RESULTS: The analytic cohort comprised 963 participants, with LVEF <50% in 74 (7.7%) and ≥50% in 889 (92.3%). Participants with LVEF<50% compared to >50% were younger (65 vs 68 years, p=0.006), more likely male (63.5% vs 44.4%, p=0.002) and of non-White race (45.9% vs 23.8%, p<0.001), and to have coronary artery disease (25.7% vs 8.9%, p<0.001) and CHF (33.8% vs 4.7%, p<0.001), higher N-terminal pro-BNP (median 487 vs 292 pg/mL, p<0.001), larger left atrial diameter index (median 2.1 vs 1.9 cm, p<0.001), and lower LVEF (median 43% vs 62%, p<0.001); P-wave terminal force in V1 was similar. Recurrent IS occurred in 10 (13.5%) patients with LVEF <50% and 61 (6.9%) with LVEF ≥ 50%. The incidence rates of recurrent stroke per 100 person-years were 7.1 (95% CI, 3.8-13.3) with LVEF <50% and 3.9 (95% CI, 3.0-5.0) with LVEF ≥ 50%. In the adjusted analysis, the risk of recurrent stroke was significantly higher with LVEF <50% vs ≥50% (HR 2.23, 95% CI 1.03-4.83). There was no significant interaction between LVEF stratum and the treatment effect (p=0.35; Figure). The risk of recurrent stroke was nominally lower among patients randomized to apixaban than aspirin with LVEF <50% (HR 0.11, 95% C.I. 0.01-1.12), and EF>50% (HR 0.87, 95% C.I. 0.52-1.45) but did not reach statistical significance.
CONCLUSION: Recurrent stroke risk was higher among patients with LVEF <50% vs ≥50%. The risk of recurrent stroke was not different among patients randomized to apixaban compared to aspirin. Further study is needed to identify the optimal anti-thrombotic treatment for patients with cryptogenic stroke and left ventricular dysfunction.
Jillella, Dinesh
(
Emory University
, Atlanta , Georgia , United States )
Sharma, Richa
(
Yale School of Medicine
, Hamden , Connecticut , United States )
Zhang, Cenai
(
Weill Cornell Medicine
, New York , New York , United States )
Elkind, Mitchell
(
COLUMBIA UNIVERSITY
, New York , New York , United States )
Kamel, Hooman
(
Weill Cornell Medicine
, New York , New York , United States )
Kronmal, Richard
(
University of Washington
, Seattle , Washington , United States )
Longstreth, W
(
HARBORVIEW MEDICAL CENTER
, Seattle , Washington , United States )
Tirschwell, David
(
HARBORVIEW MEDICAL CENTER
, Seattle , Washington , United States )
Di Tullio, Marco
(
COLUMBIA PRESBYTERIAN MED CTR
, New York , New York , United States )
Merkler, Alexander
(
Weill Cornell Medicine
, New York , New York , United States )
Nahab, Fadi
(
Emory University
, Atlanta , Georgia , United States )
Author Disclosures:
Dinesh Jillella:DO NOT have relevant financial relationships
| Alexander Merkler:No Answer
| Fadi Nahab:DO NOT have relevant financial relationships
| Richa Sharma:DO NOT have relevant financial relationships
| Cenai Zhang:DO NOT have relevant financial relationships
| Mitchell Elkind:DO have relevant financial relationships
;
Research Funding (PI or named investigator):BMS-Pfizer Alliance for Eliquis:Past (completed)
; Employee:American Heart Association:Active (exists now)
; Advisor:Atria Academy of Science and Medicine:Active (exists now)
; Royalties/Patent Beneficiary:UpToDate:Past (completed)
; Research Funding (PI or named investigator):Roche:Past (completed)
| Hooman Kamel:DO have relevant financial relationships
;
Other (please indicate in the box next to the company name):Financial disclosures for Hooman Kamel: a PI role in the ARCADIA trial, which received in-kind study drug from the BMS-Pfizer Alliance for Eliquis and ancillary study support from Roche Diagnostics; a Deputy Editor role for JAMA Neurology; clinical trial steering/executive committee roles for the STROKE-AF (Medtronic), LIBREXIA-AF (Janssen), and LAAOS-4 (Boston Scientific) trials; consulting or endpoint adjudication committee roles for AbbVie, AstraZeneca, Boehringer Ingelheim, and Novo Nordisk; and household ownership interests in TETMedical, Spectrum Plastics Group, and Ascential Technologies.:Active (exists now)
| Richard Kronmal:DO NOT have relevant financial relationships
| W Longstreth:DO NOT have relevant financial relationships
| David Tirschwell:DO have relevant financial relationships
;
Consultant:AbbVie:Past (completed)
; Research Funding (PI or named investigator):Abbott:Active (exists now)
| Marco Di Tullio:DO NOT have relevant financial relationships