Demographic and socio-economic differences in the co-occurrence of Obesity and Chronic Kidney Disease – A Population-Based Study
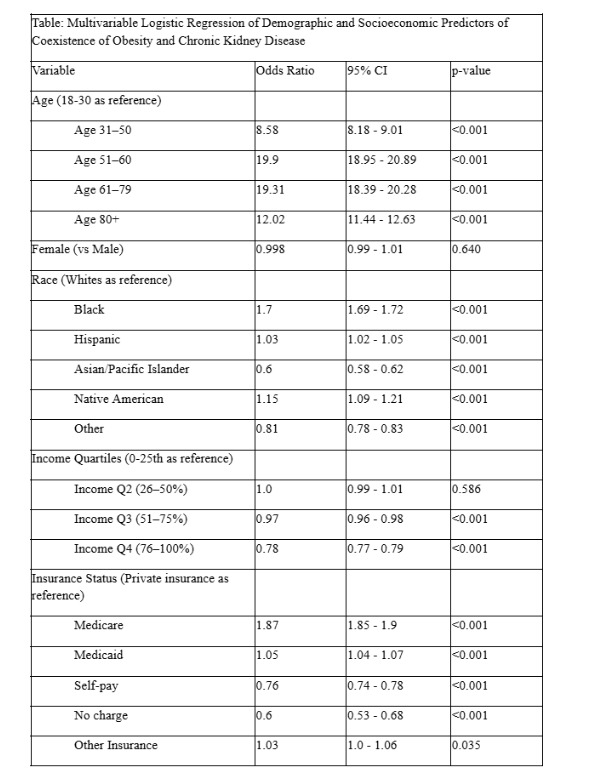
Abstract Body: Introduction Obesity is a chronic disease, with its prevalence rising globally. There is strong and consistent evidence that obesity and chronic kidney disease (CKD) frequently co-exist, with obesity being a significant and independent risk factor for the development, progression, and adverse outcomes of CKD. In this nationally represented study, we aim to identify demographic and socio-economic disparities in the co-occurrence of obesity and CKD. Methods: We performed a cross-sectional observational study using the NIS 2022 data. Adult patients with CKD and obesity were identified using the ICD-10 codes N18 and E66, respectively. A chi-square analysis was conducted to determine the variables to include. A multivariable logistic regression analysis was performed to examine demographic and social variables, with a significance level of p<0.05. All analyses were done using Stata 18.0. Results: A total of 1,059,963 patients were identified with CKD, and 1,091,389 with obesity. Of these, 256,196 patients (24%) had a co-diagnosis of both CKD and obesity. Increasing age was significantly associated with higher odds of concurrent obesity and CKD, with the highest odds observed in the 51–60 age group (OR 19.9, 95% CI: 18.95–20.89, p<0.001). Females and males had similar odds (OR 0.998, p=0.640). Compared to Whites, higher odds were seen in Black (OR 1.70, 95% CI:1.69–1.72), Hispanic (OR 1.03, 95% CI:1.02–1.05), and Native American (OR 1.15, 95% CI:1.09–1.21) populations, while Asian/Pacific Islanders (OR 0.60, 95% CI:0.58–0.62) and Others (OR 0.81, 95% CI:0.78–0.83) had lower odds (all p<0.001). Relative to the lowest income quartile, those in Q3 (OR 0.97, 95% CI:0.96–0.98) and Q4 (OR 0.78, 95% CI:0.77–0.79) had lower odds (p<0.001), while Q2 showed no difference (p=0.586). Compared to private insurance, Medicare (OR 1.87, 95% CI:1.85–1.90), Medicaid (OR 1.05, 95% CI:1.04–1.07), self-pay (OR 0.76, 95% CI:0.74–0.78), no charge (OR 0.60, 95% CI:0.53–0.68), and other insurance (OR 1.03, 95% CI:1.00–1.06) groups showed significant differences (p<0.05). Conclusions Significant demographic and socioeconomic disparities exist in the coexistence of obesity and CKD. Older age, Black and Native American race, lower income, and non-private insurance status were independently associated with higher odds. These findings highlight the need for targeted public health interventions and equitable access to preventive care and chronic disease management in high-risk populations.
Arora, Komal
(
NYMC-St Clare and St Mary
, Wallington , New Jersey , United States )
Shah, Anand
(
Rutgers NJMS
, Newark , New Jersey , United States )
Goyal, Ritik
(
Rutgers NJMS
, Newark , New Jersey , United States )
Rana, Chirag
(
NYMC-St Clare and St Mary
, Wallington , New Jersey , United States )
Author Disclosures:
Komal Arora:DO NOT have relevant financial relationships
| Anand Shah:DO NOT have relevant financial relationships
| Ritik Goyal:No Answer
| Chirag Rana:No Answer
Tahir Muhammad Waseem, Saleem Junaid, Tahir Zubia, Hamayal Muhammad, Ahmad Amna, Malik Junaid Mehmood, Nauman Haider Dr Muhammad, Ashraf Arslan, Kashif Mohammad