Hypertrophic Cardiomyopathy–Related Mortality in the United States: A 22-Year Epidemiologic Analysis of National Trends and Disparities (1999–2020)
Abstract Body: Introduction: Hypertrophic cardiomyopathy (HCM) is a heritable disorder characterized by left ventricular hypertrophy with predominant diastolic dysfunction and, in later stages, systolic impairment. It contributes to sudden cardiac death, particularly among younger individuals. While advances in diagnosis and management have improved clinical outcomes, national mortality trends and disparities in HCM-related deaths remain underexplored.
Hypothesis: We hypothesized that HCM-related mortality has declined over the past two decades in the United States but that significant disparities persist across sex, race, and geographic region.
Methods: We analyzed 20,231 mortality records from the CDC WONDER database for individuals aged >35 years from 1999 to 2020, identifying HCM (ICD-10 codes I42.1, I42.2) as the underlying cause of death. Age-adjusted mortality rates (AAMRs) per 1,000,000 were calculated. Temporal trends were assessed using Joinpoint regression to determine annual percent change (APC).
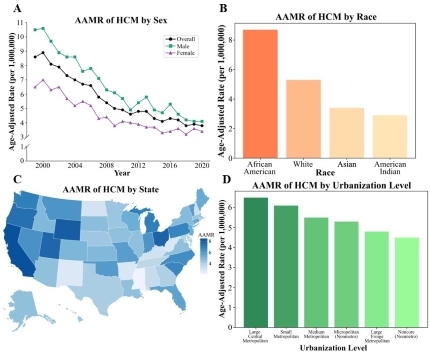
Results: From 1999 to 2020, the AAMR of HCM-related deaths decreased from 8.6 (95% CI, 8.1–9.1) to 3.8 (95% CI, 3.6–4.1), with a significant APC of –4.1% (p<0.001). Cumulative AAMR was higher in males (6.5 [95% CI, 6.3–6.6]) than females (4.5 [95% CI, 4.4–4.6]). Among racial groups, African Americans had the highest AAMR (8.7 [95% CI, 8.4–9.0]), followed by White individuals (5.3 [95% CI, 5.2–5.4]), American Indians (3.4 [95% CI, 2.7–4.0]), and Asians (2.9 [95% CI, 2.6–3.2]). Metropolitan regions had higher AAMRs than noncore rural areas (6.5 [95% CI, 6.3–6.6] vs. 4.5 [95% CI, 4.3–4.8]). The West region had the highest AAMR (7.2 [95% CI, 7.0–7.4]), followed by the Midwest (5.9 [95% CI, 5.7–6.0]), Northeast (5.3 [95% CI, 5.1–5.5]), and South (4.6 [95% CI, 4.5–4.7]).
Conclusions: Although HCM-related mortality has significantly declined over the past two decades, notable disparities remain across sex, race, and geography. The persistently higher burden among males, African Americans, and individuals in urban regions highlights the urgent need for targeted public health strategies aimed at improving early detection, equitable access to specialty care, and long-term management in high-risk communities.
Ashar, Perisa
( Duke University
, Durham
, North Carolina
, United States
)
Garg, Shriya
( University of Georgia
, Athens
, Georgia
, United States
)
Ajay Jadav, Arnav
( Washington University in St. Louis
, St. Louis
, Missouri
, United States
)
Tamirisa, Ketan
( Washington University in St. Louis
, St. Louis
, Missouri
, United States
)
Batnyam, Uyanga
( University of Washington
, Seattle
, Washington
, United States
)
Author Disclosures:
Perisa Ashar:DO NOT have relevant financial relationships
| Shriya Garg:No Answer
| Arnav Ajay Jadav:DO NOT have relevant financial relationships
| Ketan Tamirisa:No Answer
| Uyanga Batnyam:DO NOT have relevant financial relationships