Apparent Resistant Hypertension in US Adults: Temporal Trends, Renal Denervation Eligibility, and the Impact of Isolated Systolic Hypertension
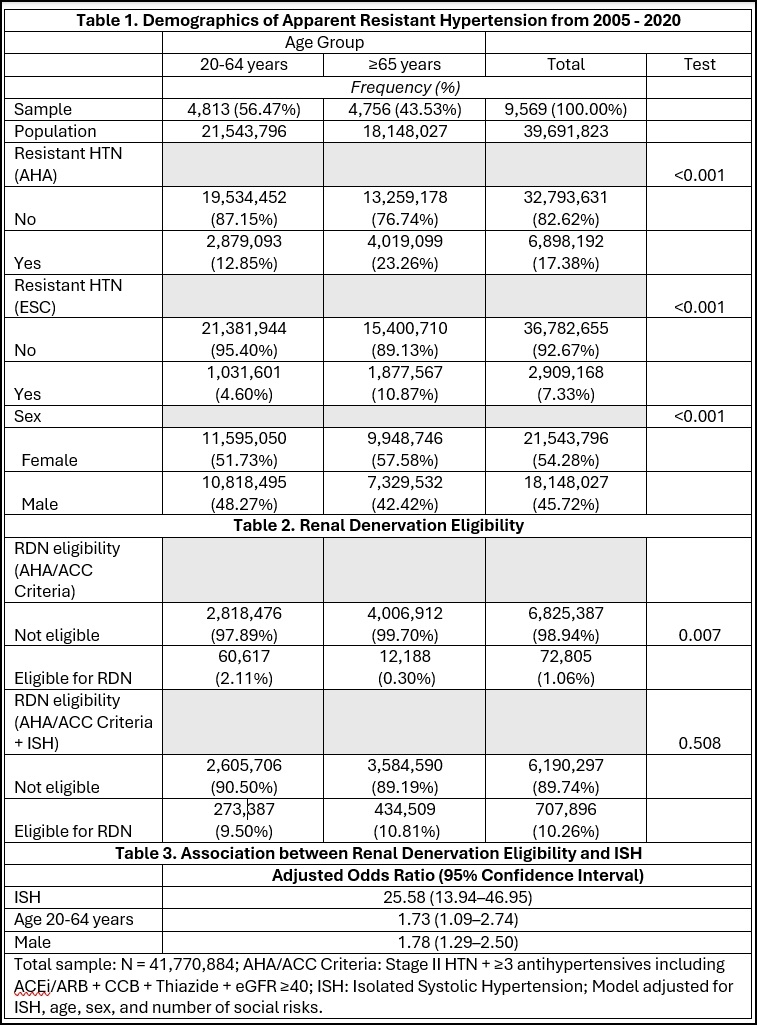
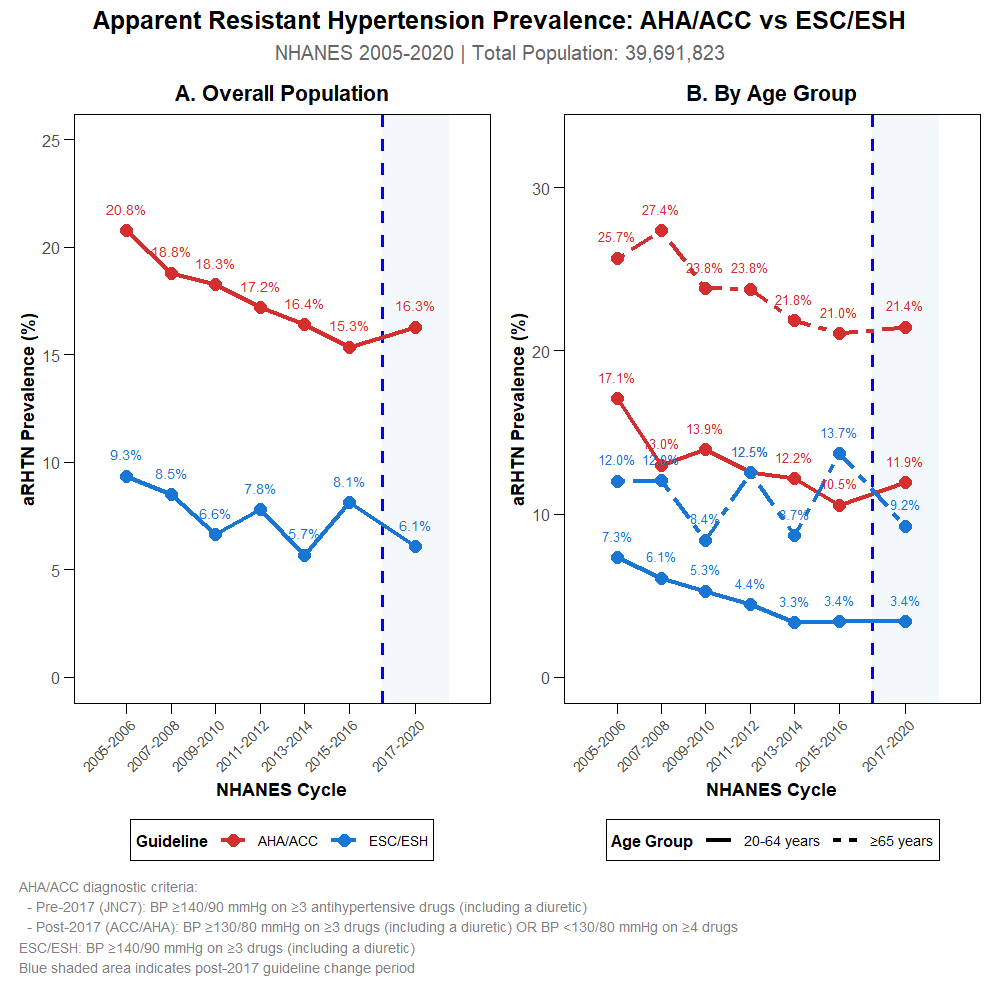
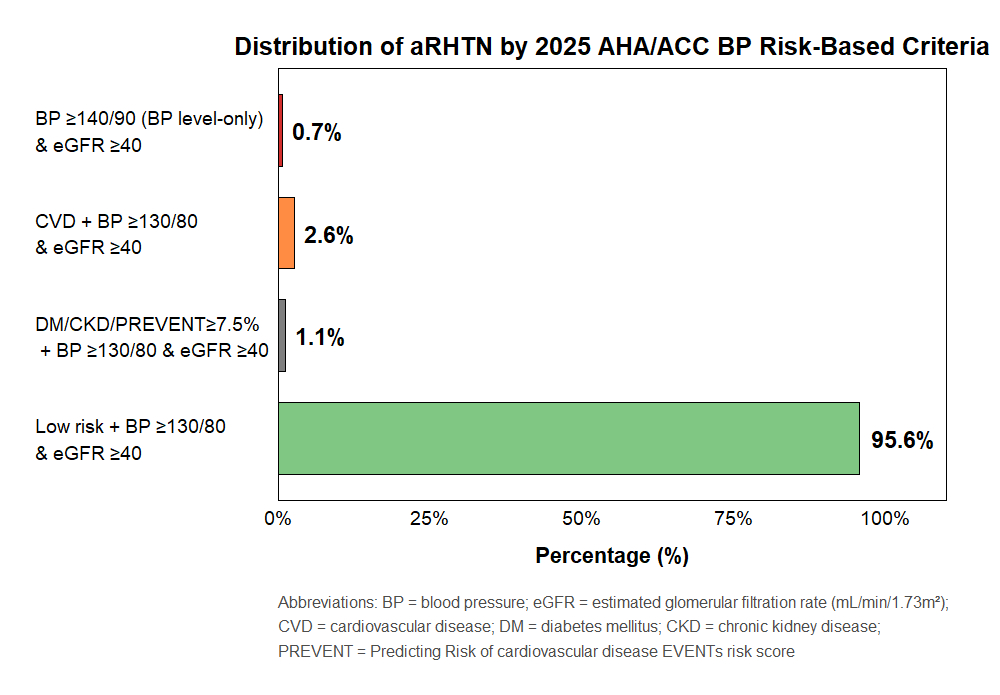
Abstract Body: Background: The 2025 AHA/ACC (American Heart Association/American College of Cardiology) and ESC/ESH (European Society of Cardiology/European Society of Hypertension) guidelines introduced new diagnostic and risk-based blood pressure (BP) thresholds, while renal denervation (RDN) has emerged as a device-based therapy for resistant hypertension. The impact of these guidelines on the prevalence, trends, and RDN eligibility among US adults with apparent resistant hypertension (aTRH) remains unclear. Methods: We analyzed adults aged ≥20 years treated for hypertension from NHANES 2005–2020. aTRH was defined by AHA/ACC (uncontrolled BP on ≥3 antihypertensive medications including a diuretic, or controlled BP on ≥4) and ESC/ESH (office BP ≥140/90 mmHg on ≥3 drug classes including a diuretic) criteria. aTRH cases were stratified by 2025 AHA/ACC risk-based thresholds. RDN eligibility was assessed using strict (SBP ≥140 and DBP ≥90 mmHg) and inclusive (including isolated systolic hypertension) criteria among patients on optimal therapy with eGFR ≥40 mL/min/1.73m2. Survey-weighted and multivariable regression analyses estimated national prevalence, temporal trends, and predictors of RDN eligibility. Results: Among 39.7 million US adults with treated hypertension, aTRH prevalence by AHA/ACC criteria declined from 21.6% (2005–06) to 16.6% (2017–20); ESC/ESH criteria yielded lower rates (6.4–9.6%). The AHA/ACC definition identified 2.4 times more cases than ESC/ESH (17.2% vs 7.3%). The prevalence was higher in adults ≥65 years versus 20–64 years (23.3% vs 12.9%, p<0.001). Multivariable regression showed older age ≥65 years (adjusted OR 1.73, 95% CI: 1.09–2.74) and male sex (OR 1.78, 95% CI: 1.29–2.50) were significantly associated with RDN eligibility. By 2025 risk stratification, 95.9% of aTRH cases were low-risk, 3.7% had CVD, 1.8% had diabetes/CKD/elevated PREVENT score, and 0.1% met BP-only criteria. Among 1,899 aTRH patients, 72,805 (1.06%) met strict RDN eligibility; inclusion of isolated systolic hypertension increased eligibility tenfold (10.26%; adjusted OR 25.58, 95% CI 8.5–12.3). Conclusions: aTRH prevalence in US adults varies substantially by guideline definition and has declined over time. Regression analysis identified age and sex as predictors of RDN eligibility. Integrating risk-based thresholds into aTRH management and expanding RDN criteria to include isolated systolic hypertension may enhance patient selection and optimize hypertension control.
Ateh Stanislas, Ketum
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Metlock, Faith
(
JOHNS HOPKINS SCHOOL OF NURSIN
, Baltimore , Maryland , United States )
Ogungbe, Bunmi
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Cingolani, Oscar
(
JOHNS HOPKINS UNIVERSITY
, Baltimore , Maryland , United States )
Commodore-mensah, Yvonne
(
JOHNS HOPKINS SCHOOL OF NURSIN
, Baltimore , Maryland , United States )