Cumulative Social Risk and Sex Differences in Hypertension Severity Among U.S. Adults: NHANES 2005–2023
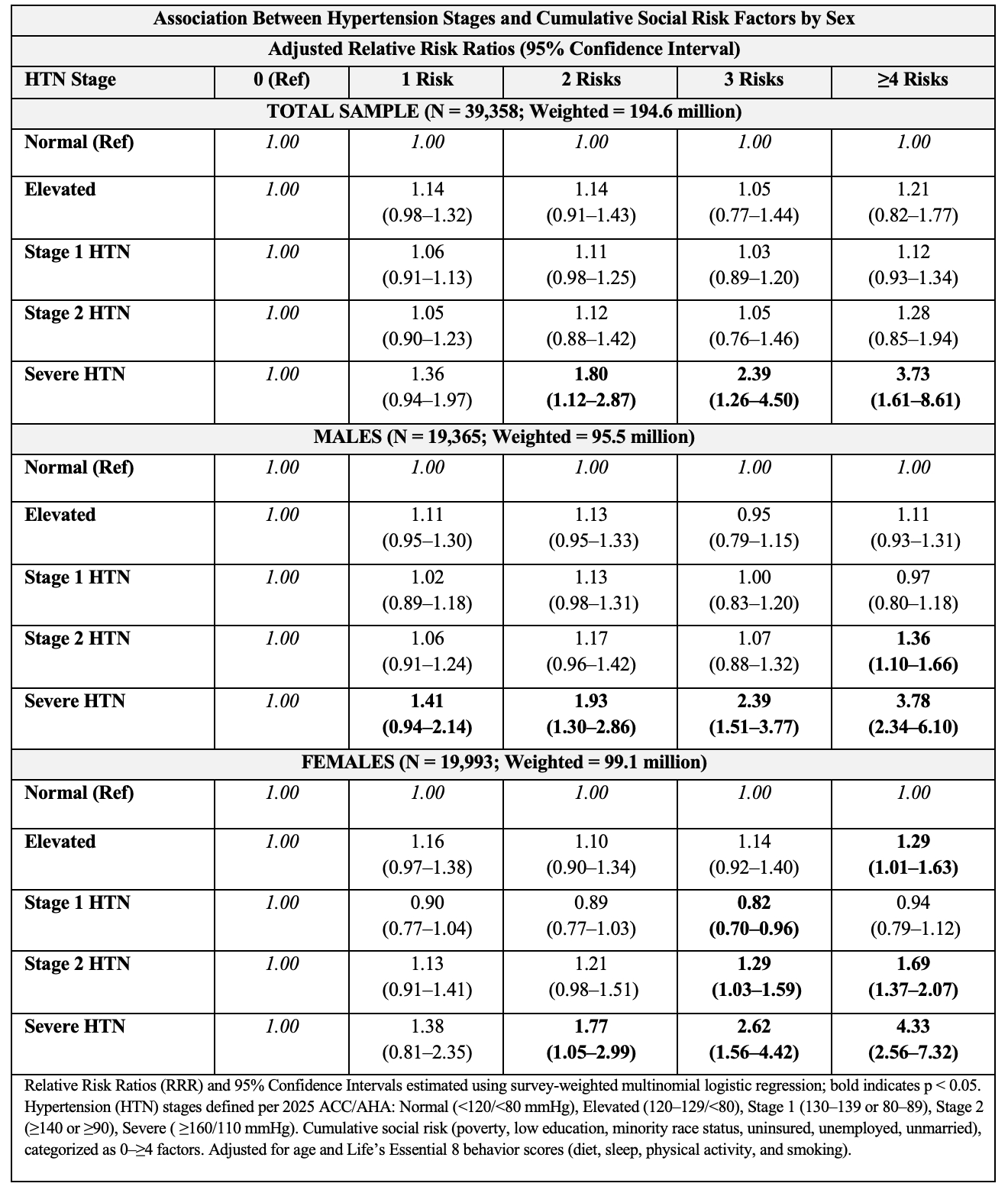
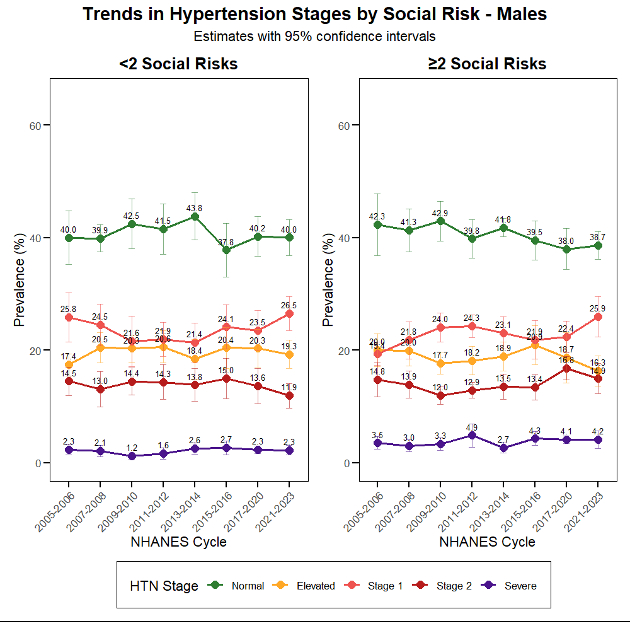
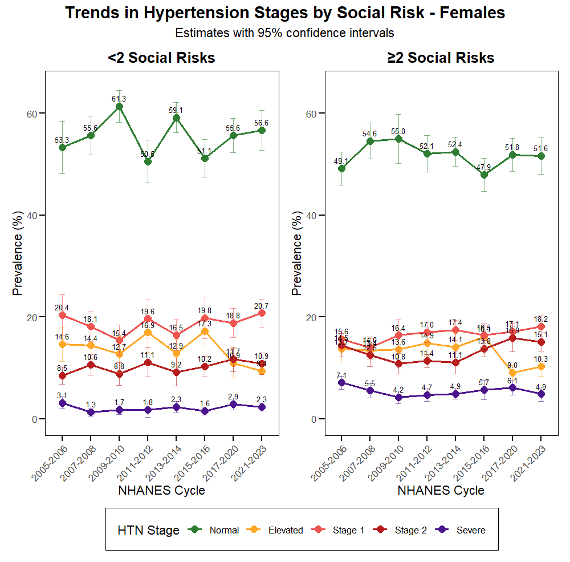
Abstract Body: Background: Social determinants of health contribute to hypertension disparities, yet the cumulative effects of multiple social risks and potential sex differences remain poorly understood. Methods: We analyzed National Health and Nutrition Examination Survey (NHANES) 2005–2023 data for adults ≥18 years. Hypertension was defined per the 2025 American College of Cardiology/American Heart Association guidelines as elevated (120–129/<80 mmHg), Stage 1 (130–139 or 80–89 mmHg), Stage 2 (140–159 or 90–109 mmHg), and severe (≥160 or ≥110 mmHg). A cumulative social risk index (0–≥4) included poverty, education, marital status, employment, insurance, and minority status. Survey-weighted multinomial logistic regression estimated adjusted relative risk ratios (aRRR) and 95% confidence interval (CIs), adjusting for age and Life’s Essential 8 behavior scores (diet, sleep, physical activity, and smoking). Analyses were stratified by sex, and temporal trends were evaluated across NHANES cycles using ≥2 social risks as the threshold, reflecting the population median. Results: Among 194.6 million adults (N = 39,358), mean age was 47.7 years, and 44% had ≥2 social risks (46% females, 41% males). In the total population, cumulative social risk was not associated with elevated, Stage 1, or Stage 2 hypertension; however, ≥4 risks were associated with severe hypertension (aRRR = 3.73, 95% CI 1.61–8.61). Among males, associations appeared only at advanced stages: Stage 2 (aRRR = 1.36, 95% CI 1.10–1.66) and severe hypertension (aRRR = 3.78, 95% CI 2.34–6.10). Among females, cumulative social risk showed a progressive pattern: Stage 1 hypertension was lower at three risks (aRRR = 0.82, 95% CI 0.70–0.96), while Stage 2 risk emerged at three risks (aRRR = 1.29, 95% CI 1.03–1.59), and at four or more risks, both elevated BP (aRRR = 1.29, 95% CI 1.01–1.63) and severe hypertension (aRRR = 4.33, 95% CI 2.56–7.32) were significantly higher. Over time, adults with ≥2 social risks showed widening disparities—males experienced rising Stage 2 and severe hypertension in later cycles, while females demonstrated earlier, sustained increases beginning at Stage 1. Conclusions: Cumulative social disadvantage was independently associated with more severe hypertension, with stronger and earlier effects among females. Despite stable national hypertension trends, persistent social and sex inequities underscore the need for upstream interventions to achieve equitable blood pressure control in the U.S.
Metlock, Faith
(
Johns Hopkins University
, North Bethesda , Maryland , United States )
Ateh Stanislas, Ketum
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Ogungbe, Bunmi
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Hinneh, Thomas
(
Johns Hopkins University
, Baltimore , Maryland , United States )
Commodore-mensah, Yvonne
(
JOHNS HOPKINS SCHOOL OF NURSIN
, Baltimore , Maryland , United States )