Electronic Patient Portal Recruits for Cardiovascular Trials are Demographically Distinct with Improved Rates of Eligibility and Screening Attendance
Abstract Body: Introduction Participant recruitment challenges are a leading cause of delays and early termination in clinical trials, resulting in substantial financial costs and risk of underpowered, unrepresentative samples. Recruitment through patient messaging on the electronic medical record (EMR) provides a time- and cost-effective option. However, research on the EMR’s effectiveness in enrolling a representative sample is sparse.
Hypothesis Participant demographics, eligibility, and screening attendance will differ between EMR recruitment and traditional recruitment methods in two similar randomized control trials (GoFresh, GoFreshRx).
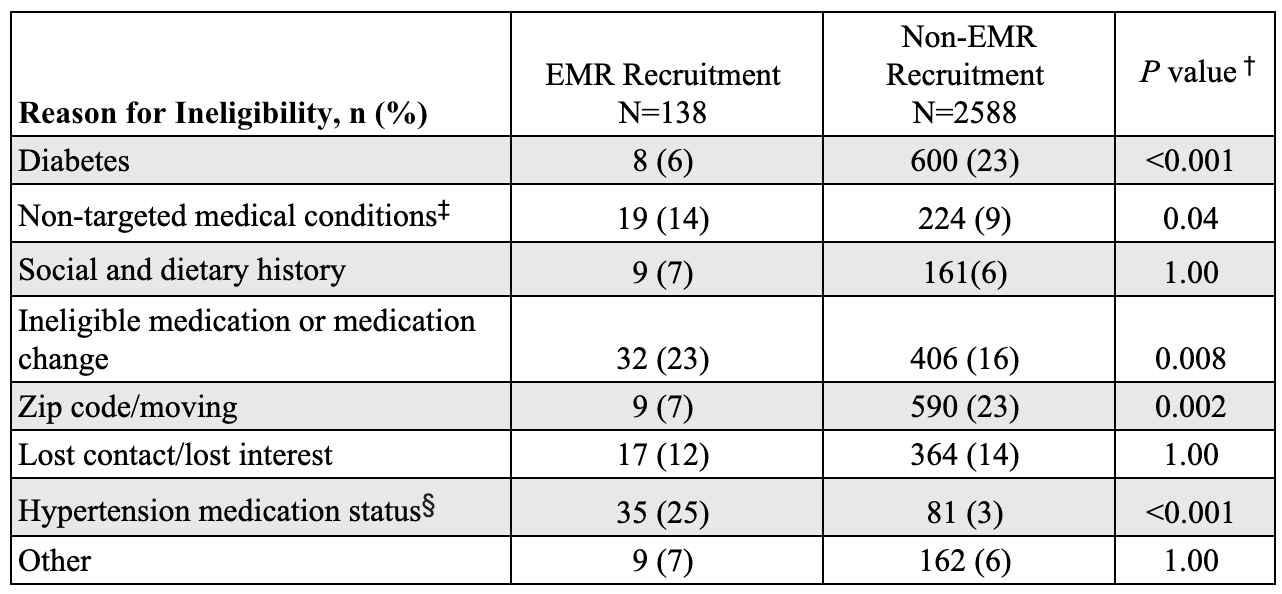
Methods Trials for a lifestyle intervention used EMR, flyers, and other methods to recruit Black adults (≥18 years) with high blood pressure living in Boston-area food deserts. EMR recruitment included additional medication criteria. Participants completed a telephone pre-screen (PQ) and, if eligible, two in-person screenings (SVa, SVb). Outcomes included participant demographics, pre-screen eligibility (i.e., eligible after PQ), screening attendance (i.e., attending SVa), and post-screen eligibility (i.e., eligible after SVa/SVb). Multivariable logistic regressions modeled outcomes by recruitment source (EMR vs. non-EMR), adjusting for age and hypertension treatment status (participants in GoFreshRx, but not GoFresh, were on treatment). We compared ineligibility reasons between EMR and non-EMR recruits using chi-square tests with Bonferroni-corrected post-hoc pairwise comparisons.
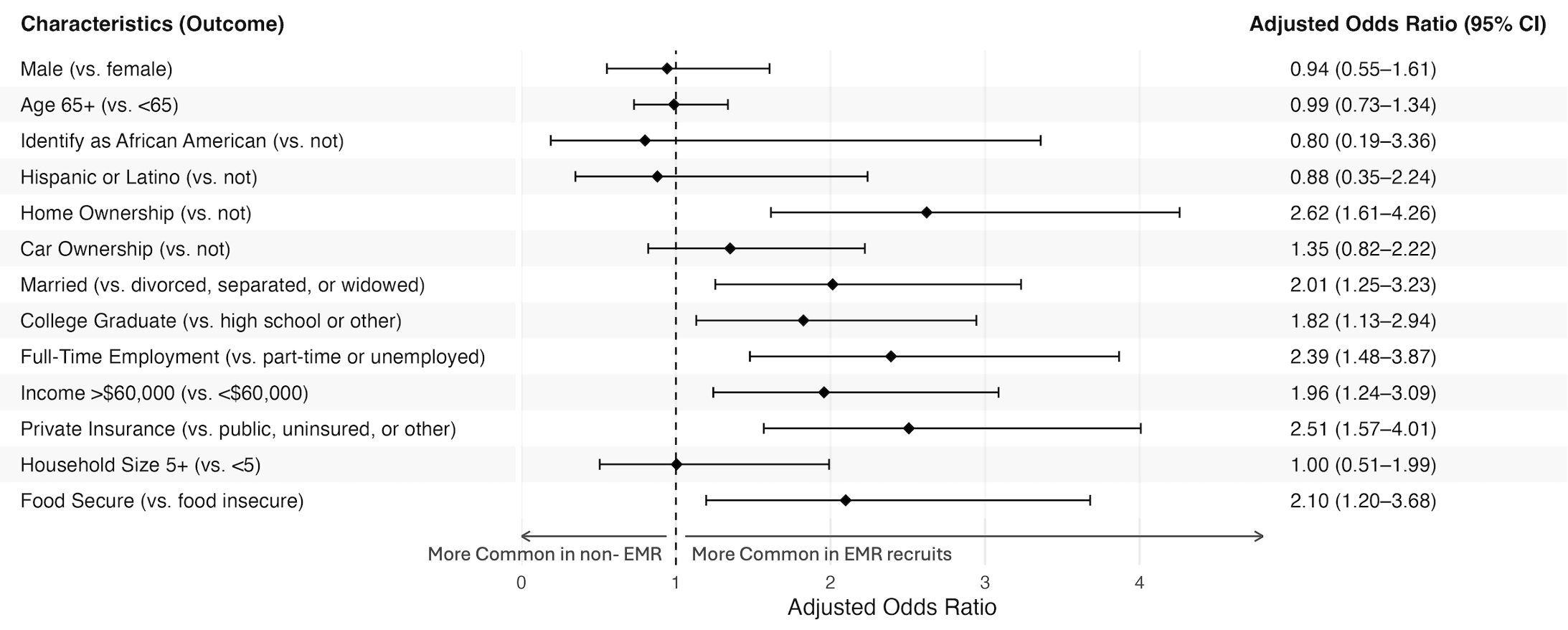
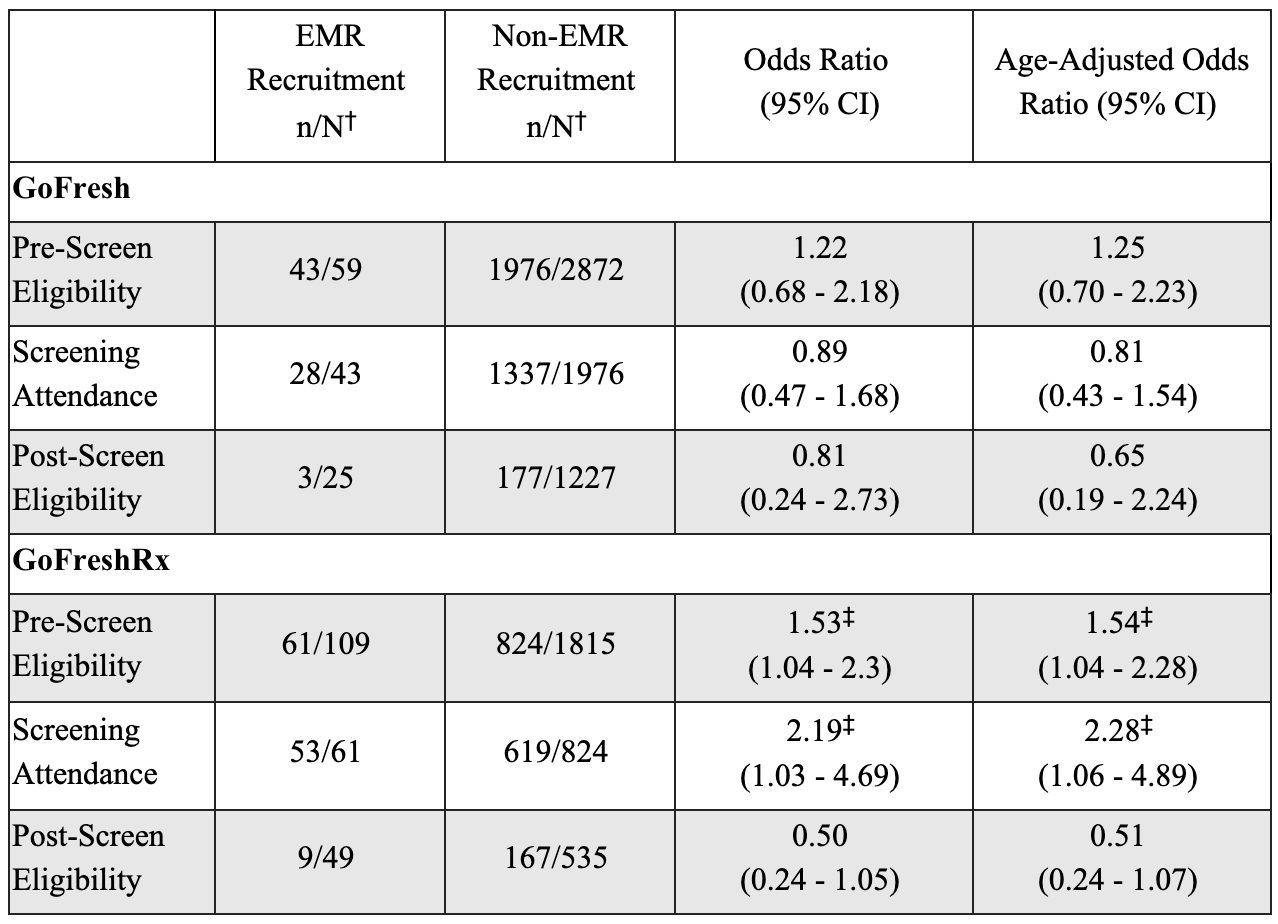
Results People recruited by EMR were more likely to own their home, be married, be a college graduate, be employed full-time, have a household income >$60,000, have private health insurance, and be food secure (all P<0.05; Figure 1). In GoFreshRx, EMR recruits had greater odds of pre-screen eligibility (Adjusted Odds Ratio [aOR]: 1.54; 95% CI: 1.04, 2.28) and screening attendance (aOR: 2.28, 95% CI: 1.06, 4.89; Table 1). Disqualifying medical conditions, particularly diabetes, accounted for a lower proporton of reasons for ineligibility in EMR than in non-EMR recruited populations (P<0.001; Table 2).
Conclusion EMR recruitment offers opportunities for more targeted recruitment with greater eligibility rates than other recruitment methods. It can successfully recruit underrepresented minoritized populations; however, EMR recruits were of higher socioeconomic status. Thus, combining EMR use with other approaches may be necessary to achieve representative samples.
Lee, Grace
(
Harvard Medical School
, Brookline , Massachusetts , United States )
Wu, Yingfei
(
BIDMC
, Boston , Massachusetts , United States )
Cao, Jingyi
(
BIDMC
, Boston , Massachusetts , United States )
Grobman, Benjamin
(
Harvard Medical School
, Boston , Massachusetts , United States )
Col, Hannah
(
BIDMC
, Boston , Massachusetts , United States )
Gao, Katie
(
Harvard Medical School
, Brookline , Massachusetts , United States )
Carranza Celis, Jose
(
Harvard Medical School
, Brookline , Massachusetts , United States )
Zhang, Mingyu
(
Harvard Medical School
, Boston , Massachusetts , United States )
Aidoo, Emily
(
BIDMC
, Boston , Massachusetts , United States )
Budu, Marian
(
Beth Israel Deaconess Medical Ctr.
, Boston , Massachusetts , United States )
Larbi, Fredrick
(
Beth Israel Deaconess Medical Ctr
, Boston , Massachusetts , United States )
Ferro, Kayla
(
BIDMC
, Boston , Massachusetts , United States )
Patil, Dhrumil
(
BIDMC
, Boston , Massachusetts , United States )
Plante, Timothy
(
University of Vermont
, Burlington , Vermont , United States )
Juraschek, Stephen
(
BIDMC-Harvard Medical School
, Boston , Massachusetts , United States )