Effect of Spironolactone versus Alpha or Beta Blockers on Systolic BP in Patients with Resistant Hypertension
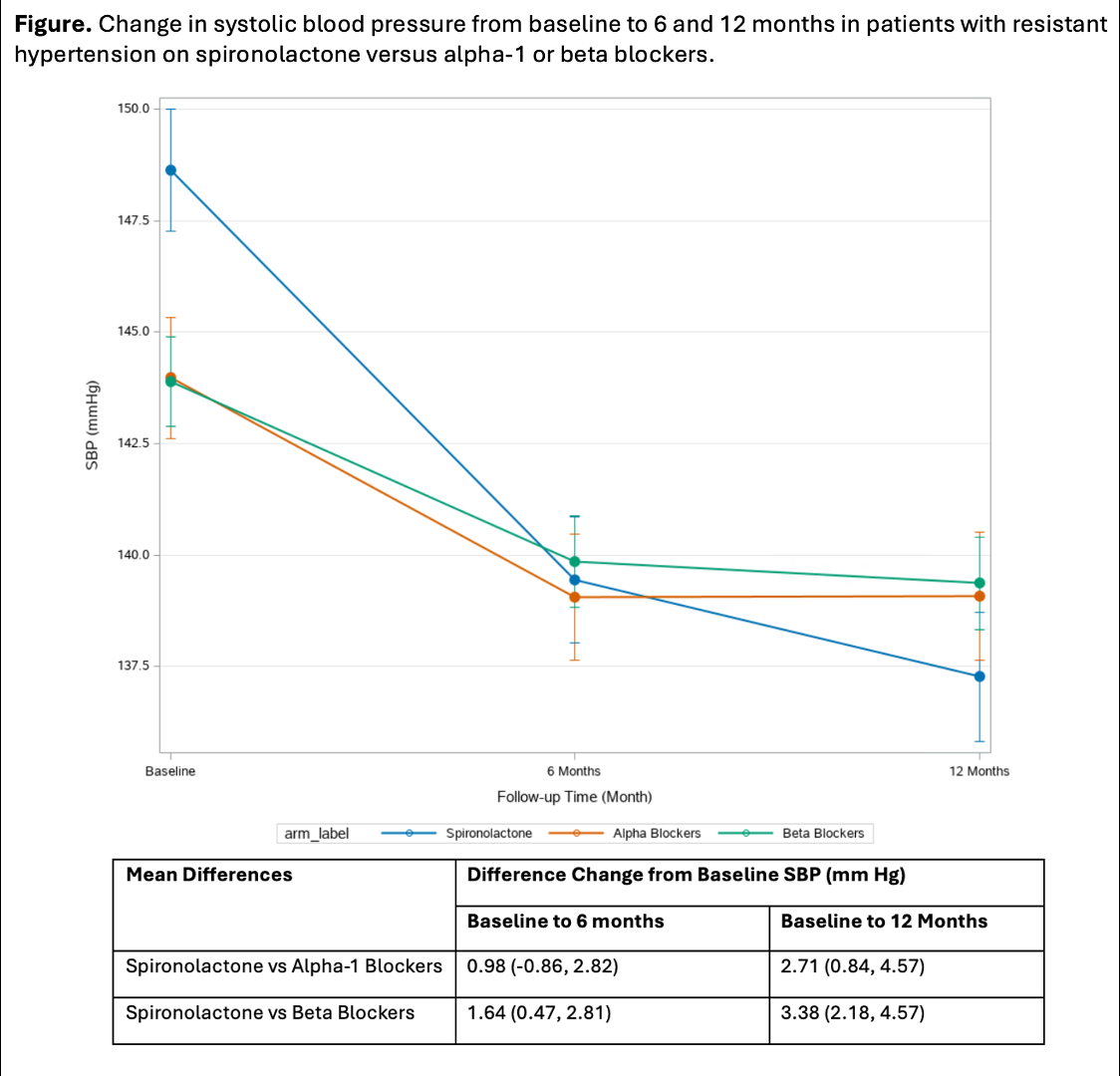
Abstract Body: Introduction. The optimal fourth-line drug therapy for resistant hypertension remains uncertain. We emulated a target trial of initiating spironolactone versus an alpha or beta blocker as an add-on therapy on blood pressure (BP) control in patients with resistant hypertension (RH). Methods. We emulated sequential trials for adults with resistant hypertension, defined as having a systolic BP > 130 mm Hg while concurrently on three classes of anti-hypertensive medication. We included patients in the Veterans Health Administration (VA) who met eligibility criteria between 2016 and 2022 who initiated one of three add-on medications for treatment of RH: spironolactone, an alpha-1 blocker, or a beta blocker. We applied inverse probability of treatment weights using >50 baseline covariates to approximate randomization. The outcome of interest was the difference in change in systolic BP from baseline to 6 months and baseline to 12 months between spironolactone and other drug classes, estimated through a weighted linear mixed effects model. Results. Among 918 adults who initiated spironolactone, 916 adults who initiated an alpha-1 blocker, and 3690 patients who initiated a beta blocker (mean age 67.6 years [SD, 9.7], mean systolic BP 146.7 mm Hg [SD, 13.1]), the average duration of continuous treatment was 14.7 months (SD, 9.5), 11.7 months (SD, 9.8), and 15.8 (SD, 9.6) months respectively. The change in systolic BP from baseline to 6 and 12 months was 7 mm Hg (95% CI, 6, 8) and 9 mm Hg (8, 11) respectively for spironolactone; 6 mm Hg [5, 7] and 7 mm Hg [5, 8]) for an alpha 1 blocker; and 5 mm Hg [4, 6] and 5 mm Hg [4, 6]) for a beta blocker. The difference between change in systolic BP at 12 months between spironolactone versus an alpha-1 blocker or beta blockers was significantly larger for spironolactone at 12 months (vs alpha-1 blockers, 3 mm Hg [1, 5]; vs beta blockers, 3 mm Hg [2, 5]). Conclusions. Spironolactone was more effective add-on fourth-line therapy for systolic BP lowering in the treatment of RH, supporting findings from PATHWAY-2 in a larger population with more comorbidity.
Li, June
(
Stanford University
, Stanford , California , United States )
Montez-rath, Maria
(
Stanford University
, Stanford , California , United States )
Odden, Michelle
(
Stanford University
, Palo Alto , California , United States )
Tamura, Manjula
(
Stanford University
, Stanford , California , United States )