Effect of Expanded Child Tax Credit Advance Payments on Population Gestational Diabetes Rates: A Quasi-Experimental Analysis
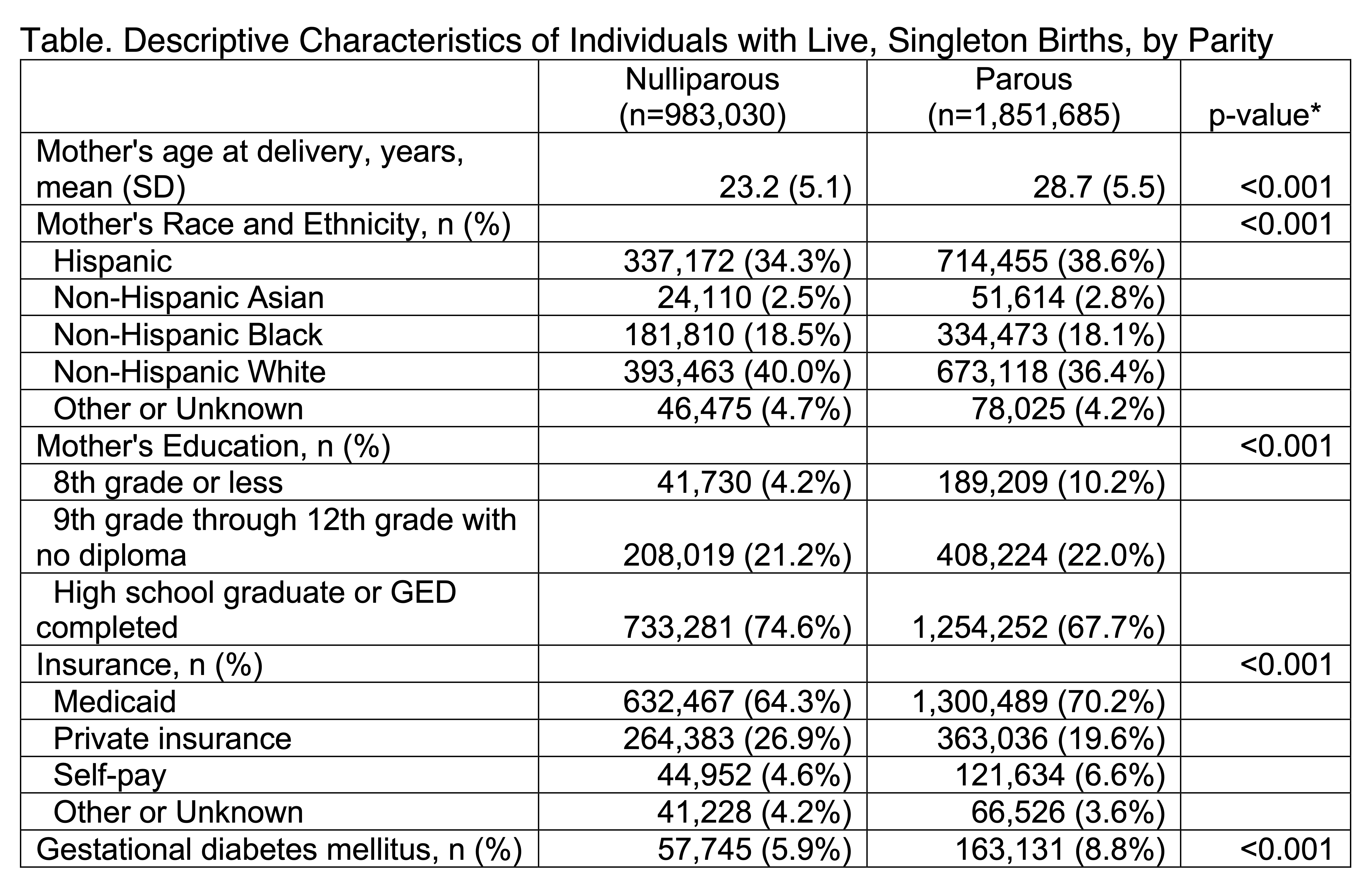
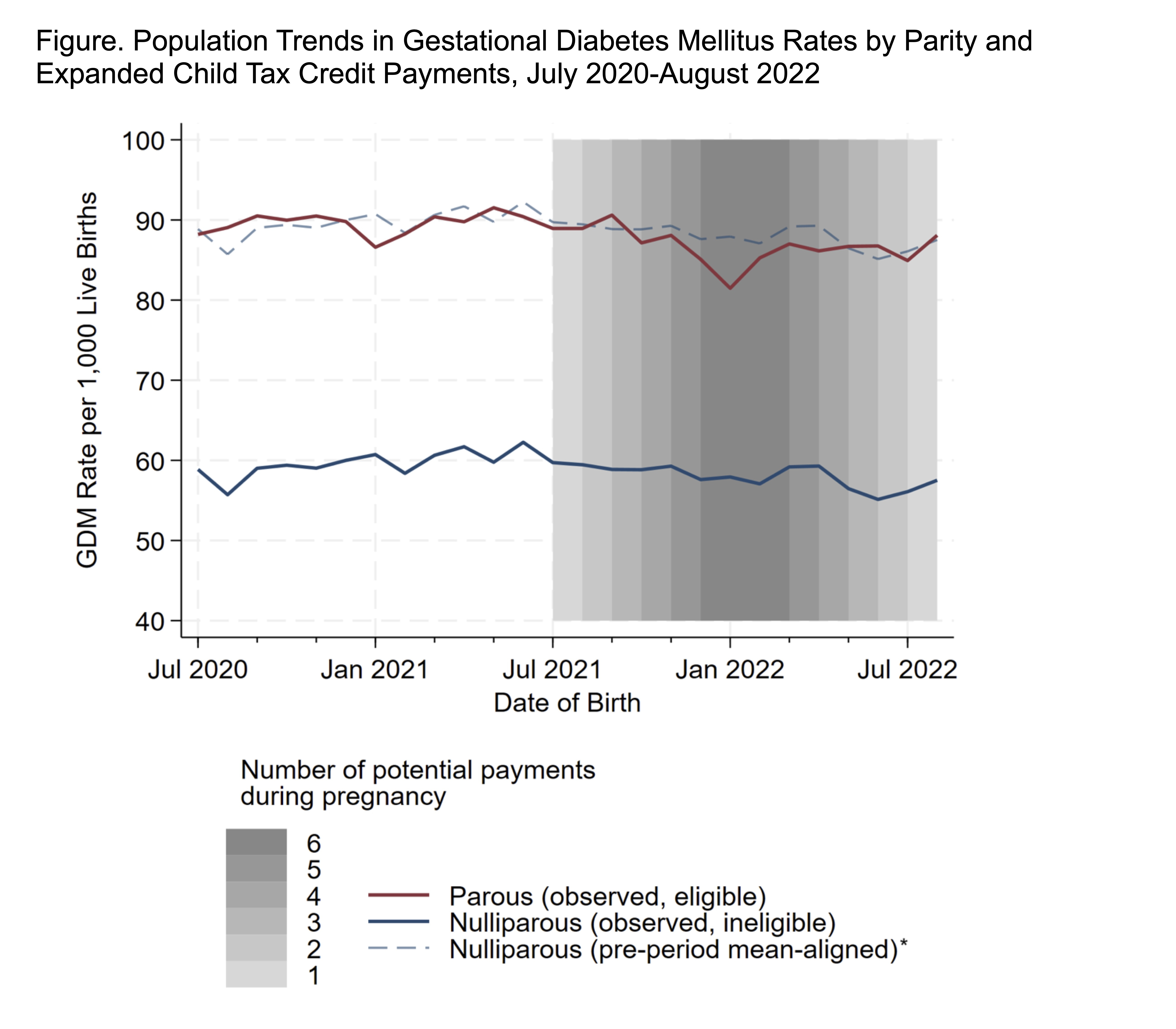
Abstract Body: Background: The temporary expansion of the federal Child Tax Credit (CTC) under the American Rescue Plan provided monthly advance payments to eligible families with children between July and December 2021 in the US. We used quasi-experimental methods to understand the effect of expanded CTC advance payments on rates of gestational diabetes mellitus (GDM). Methods: Using serial monthly cross-sectional US birth certificate data from the National Center for Health Statistics, we evaluated US residents aged 15-44 years who had a live birth between July 1, 2020 to August 31, 2022. We included individuals with a singleton birth, with available GDM and live birth order data, and with a high school education level or less since most would be eligible for CTC advance payments. Differences-in-differences linear probability models were used to evaluate the effects of ≥1, ≥4, or 6 (the maximum possible) advance payments received during pregnancy on population-level GDM rates. Analyses compared parous (likely eligible for CTC payments) and nulliparous (likely ineligible for CTC payments) individuals before (July 2020-June 2021) and after advance payments were disbursed (≥1 payment: July 2021-August 2022; ≥4 payments: October 2021-May 2022; 6 payments: December 2021-March 2022). Linear regression was used to evaluate the association of number of advance payments during pregnancy and GDM rate. Models controlled for maternal age, maternal race and ethnicity, and insurance type. Results: Among 2,834,715 births, 65.3% were to parous individuals. The overall GDM rate was 77.9 per 1000 births. There was a graded association between receiving advance payments during pregnancy and lower GDM rates: a reduction of 1.4 (95% CI, -2.7, -0.2) GDM cases per 1000 births among those who were eligible for ≥1 payment; a reduction of 2.6 (95% CI, -4.0, -1.2) GDM cases per 1000 births for those eligible for ≥4 payments; and a reduction of 3.5 (95% CI, -5.3, -1.7) GDM cases per 1000 births for those eligible for 6 payments. Between July 2021 and August 2022, each additional month of payments during pregnancy was associated with a 0.75 (95% CI, -1.05, -0.45) per 1000 births-lower GDM rate. Conclusions: Advance payments from the expanded CTC were associated with dose-dependent reductions in population GDM rates among parous individuals with a high school education or less. Economic assistance to families may promote health during pregnancy.
Lam, Emily
(
Northwestern University
, Chicago , Illinois , United States )
Huang, Xiaoning
(
Northwestern University
, Chicago , Illinois , United States )
Shah, Nilay
(
Northwestern University
, Chicago , Illinois , United States )