Association between AHA’s Life’s Essential 8 and Coronary Artery Plaque Burden in the VA Million Veteran Program
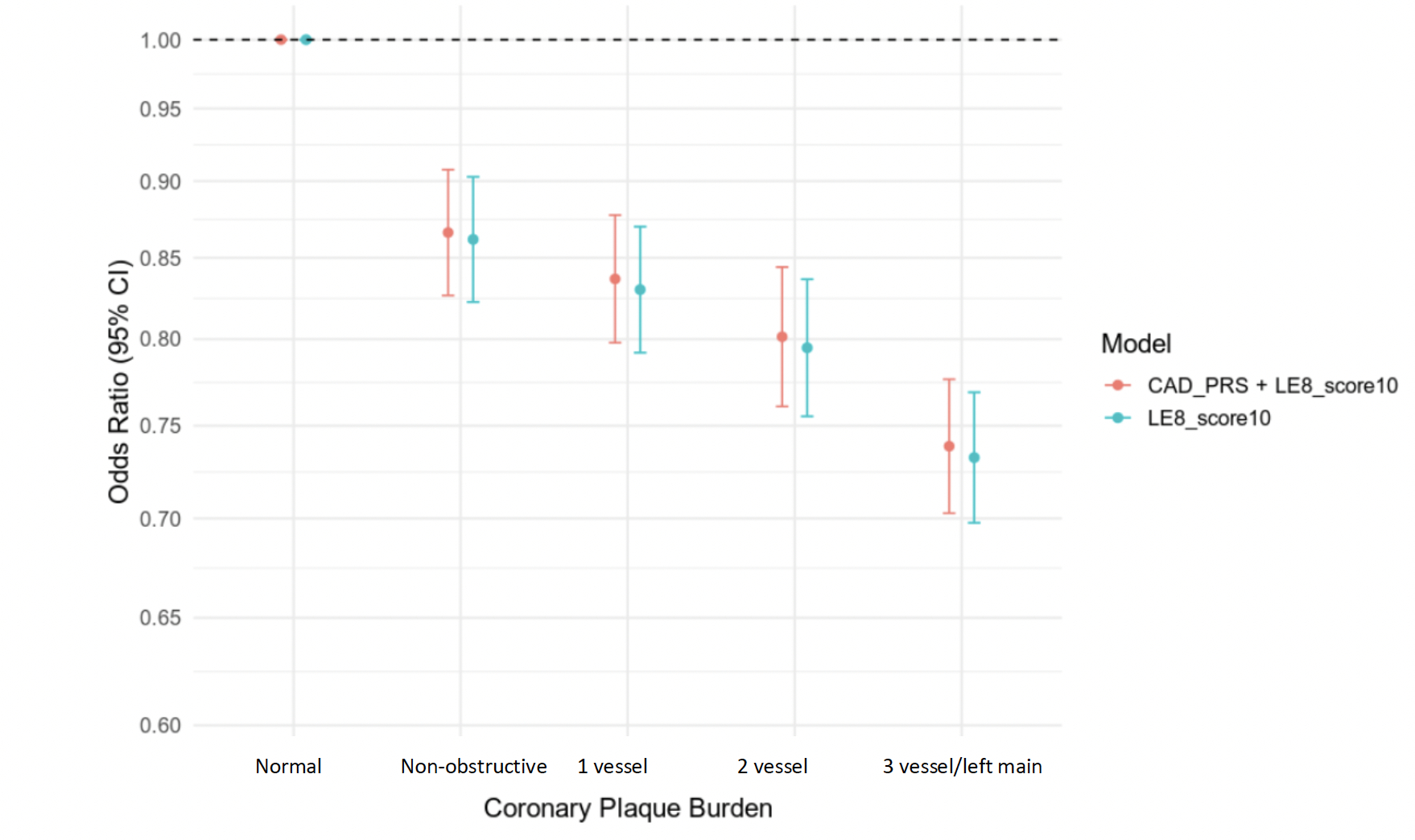
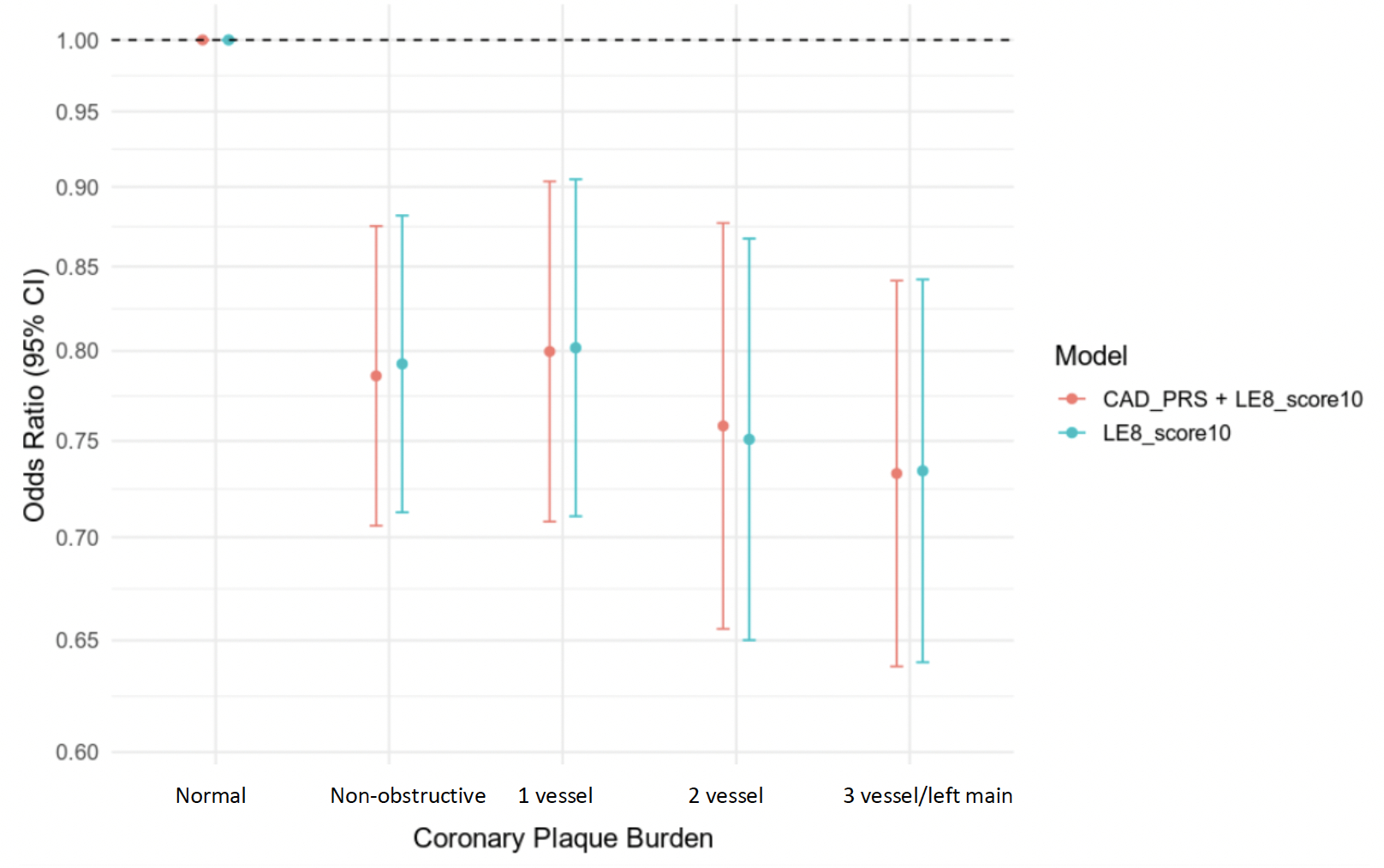
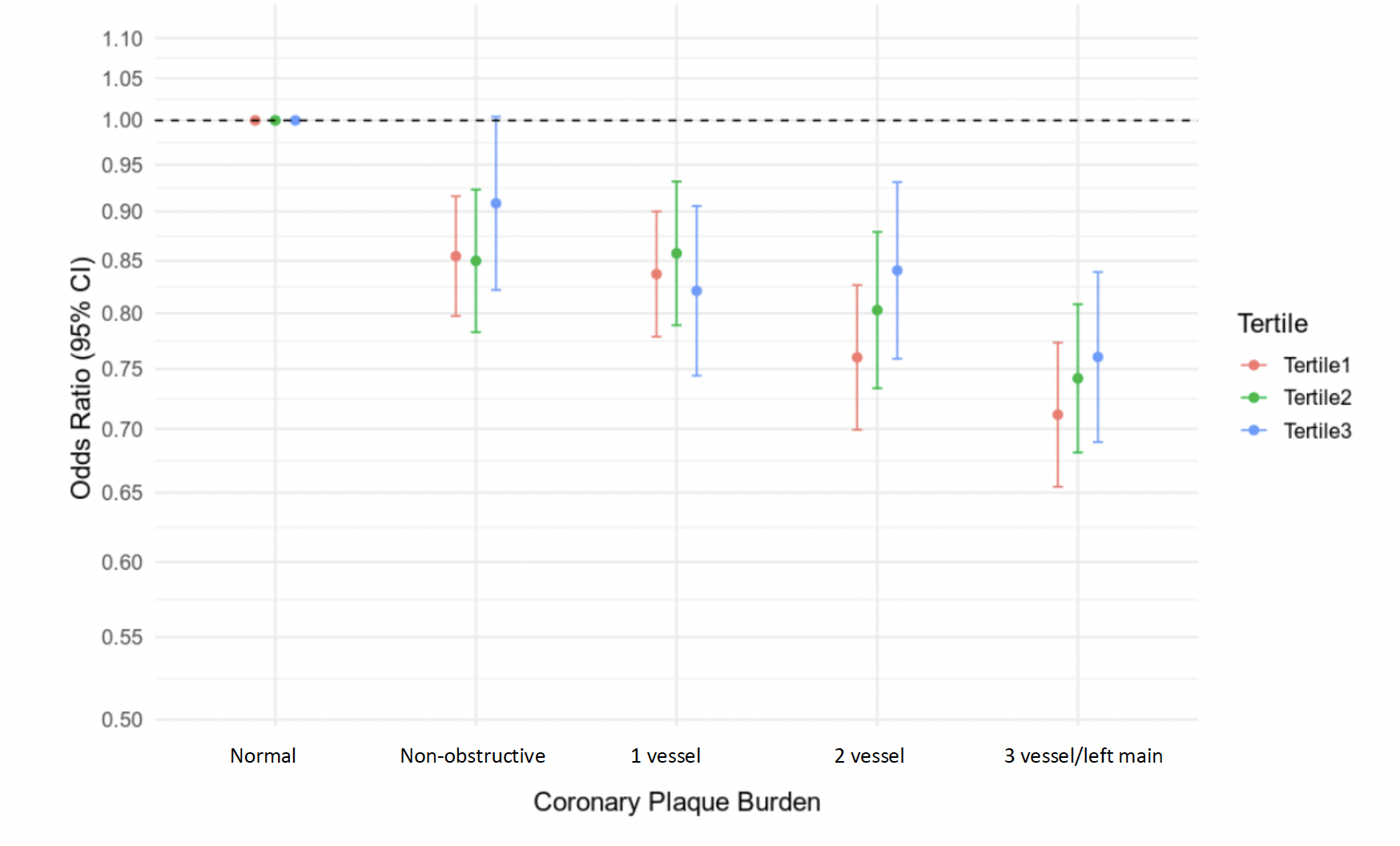
Abstract Body: Background: While AHA’s Life’s Essential 8 (LE8) metric predicts cardiovascular events, its association with coronary plaque measured by invasive angiography and interaction with genetic risk are unknown. We examined associations between LE8, plaque burden, and genetically predicted coronary artery disease (CAD) in U.S. veterans. Methods: This cohort study included VA Million Veteran Program (MVP) participants who underwent invasive angiography (2000-2021) and completed the MVP Lifestyle Survey to derive the exposure LE8 score (0-100; higher = better cardiovascular health). The outcome was plaque severity (normal = reference, non-obstructive, 1-vessel, 2-vessel, 3-vessel/left main disease). Multinomial regression was used to assess associations between LE8 and plaque severity, adjusting for age at angiogram, sex, race, and ethnicity. We also examined whether the effects of LE8 on plaque severity are independent of genetically predicted CAD estimated by a polygenic risk score. Results: We included 22,234 veterans (mean [SD] age, 67.4 [8.4] years; 21,447 [96.5%] male); 18,304 (82.3%) self-identified as White and 2,186 [9.8%] as Black. Median [IQR] LE8 score was 54 [45-63]. LE8 score was inversely associated with prevalence of any plaque, with larger effect sizes observed with increasing plaque burden: OR per 10 points increase in LE8 score was 0.86 (P = 9.2×10-15) for non-obstructive, 0.84 (P = 5.8×10-20) for 1-vessel, 0.81 (P = 6.7×10-24) for 2-vessel, and 0.74 (P = 1.6×10-50) for 3-vessel/left main disease. Cholesterol, glucose, and smoking were the LE8 components most strongly associated with plaque burden. Among 15,015 participants of genetically inferred European ancestry (EUR) and 1,825 of African ancestry (AFR), LE8 score remained inversely associated with plaque burden independent of genetically predicted CAD. We did not detect a significant interaction between LE8 and genetic risk for CAD, but we observed a trend towards attenuated LE8 effects for those with high genetic risk among EUR (P interaction = 0.095). Conclusions: Higher LE8 score is associated with lower odds of developing coronary artery plaque, with stronger associations across greater plaque burden, independent of genetically predicted CAD. Among individuals with lower genetic risk for CAD, LE8 was more strongly associated with plaque burden. These findings highlight the value of lifestyle-based interventions to mitigate plaque accumulation even in those with genetic predisposition.
Huang, Rose
(
VA BOSTON HEALTHCARE SYSTEM
, Boston , Massachusetts , United States )
Hilliard, Austin
(
Stanford University-VAPAHCS
, Los Altos , California , United States )
Tsao, Philip
(
Stanford University-VAPAHCS
, Los Altos , California , United States )
Assimes, Themistocles
(
Stanford University-VAPAHCS
, Los Altos , California , United States )
Clarke, Shoa
(
Stanford University-VAPAHCS
, Los Altos , California , United States )