United States Climate Vulnerability Index and Atherosclerotic Cardiovascular Disease Risk Prediction
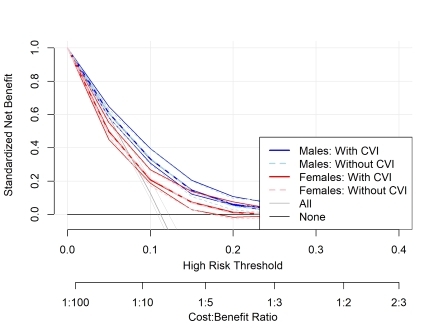
Abstract Body: Introduction: Climate-amplified weather events are known to increase Atherosclerotic Cardiovascular Disease (ASCVD) risk, particularly coronary heart disease (CHD) – the most common form of ASCVD. The U.S. Climate Vulnerability Index (CVI) is a novel summary metric of 184 health, infrastructure, and socioeconomic measures that represent community-level vulnerabilities to climate risks, allowing us to quantify the impact of climate change on health outcomes. In this study, we created a CVI-modified PREVENT model for ASCVD and compared it to the Base PREVENT models. Hypothesis: Adding CVIs to PREVENT models improves the accuracy and calibration of 10-year ASCVD risk prediction. Methods: We utilized the REasons for Geographic and Racial Differences in Stroke- Myocardial Infarction cohort, which includes 30,239 adults aged ≥ 45 years from 48 contiguous states enrolled 2003-07 who were followed for 10+ years. We applied the PREVENT equations to REGARDS-MI data using cause-specific Cox models with multiple imputation to predict 10-year ASCVD risk. Bootstrapping was used to estimate c-statistics, calibration slopes, and 95% confidence intervals. Standardized net benefit was used to approximate clinical utility. Results: Our sample included 23,678 participants (41% male; 42% Black, median age: 64) without ASCVD. Over a median 10 years, we observed 2081 ASCVD, 1207 CHD, and 970 stroke events. C-statistics and calibration slopes for CVI-modified and original PREVENT models were similar: FemaleCVI 0.73 (0.71, 0.74) and calibration slope: 0.95 (0.88, 1.04) vs FemaleNoCVI 0.72 (0.70, 0.74) and calibration slope: 0.96 (0.88, 1.05) | MaleCVI 0.69 (0.67, 0.70) and calibration slope: 0.94 (0.86, 1.03) vs MaleNoCVI 0.68 (0.67, 0.70) and calibration slope 0.95 (0.87, 1.04). Adding the CVI yielded clinically meaningful utility at low thresholds (i.e. 5%) for females compared the current PREVENT models in the prediction of ASCVD, but does not improve prediction for males. We observed similar patterns for stroke and CHD outcomes. Conclusions: Adding CVI to the PREVENT equations resulted in only minor improvements in accuracy and calibration, which may be due to use of area-level measures for climate change. We note small changes in the standardized net benefit for females compared to males with inclusion of CVI.
Russo, Lindsey
(
Weill Cornell Medicine
, Sleepy Hollow , New York , United States )
Pinheiro, Laura
(
Weill Cornell Medicine
, New York , New York , United States )
Whitcomb, Brian
(
University of Massachusetts Amherst
, Amherst , Massachusetts , United States )
Tee Lewis, Grace
(
Environmental Defense Fund
, Houston , Texas , United States )
Quezada-pinedo, Hugo G
(
Duke University
, Durham , North Carolina , United States )
Nahid, Musarrat
(
Weill Cornell Medicine
, Sleepy Hollow , New York , United States )
Abadi, Azar
(
University of Alabama at Birmingham
, Birmingham , Alabama , United States )
Levitan, Emily
(
UNIVERSITY ALABAMA AT BIRMINGHAM
, Birmingham , Alabama , United States )
Al-kindi, Sadeer
(
Houston Methodist
, Houston , Texas , United States )
Safford, Monika
(
WEILL CORNELL MEDICINE
, New York , New York , United States )
Ghosh, Arnab
(
Weill Cornell Medicine
, Sleepy Hollow , New York , United States )